Disc Biacuplasty: A Patient's Guide to Spinal Pain Relief
Some readers arrive here after months, sometimes years, of the same discouraging routine. You stretch in the morning, feel that familiar ache in your low back before your feet fully hit the floor, try physical therapy, try medication, maybe even try an injection, and still the pain keeps narrowing your life. Sitting through dinner becomes work. Travel feels strategic. Exercise turns into avoidance.
When back pain behaves like that, the right question isn't only “How do I calm it down?” It's also “What structure is causing it?” For a specific group of patients, the answer is the spinal disc itself. That's where Disc Biacuplasty enters the conversation. It's a minimally invasive procedure designed for discogenic pain, meaning pain generated from a damaged disc rather than from a pinched nerve or an arthritic joint.
Ending the Cycle of Chronic Disc Pain
A common story goes like this. A patient develops low back pain after lifting, sports, long commuting, or no obvious trigger at all. Early on, the pain seems manageable. Then it stops behaving like a short-term injury. It lingers, flares with sitting, and returns the moment activity increases. Standard treatments help a little, but not enough to restore confidence.
That experience is frustrating because chronic low back pain isn't one condition. It's a category. Muscles can hurt. Facet joints can hurt. Nerves can hurt. Discs can hurt. When those causes get blended together, patients often receive broad advice instead of precise care. If your symptoms haven't improved with the basics, a more targeted evaluation may be the missing step. Our overview of chronic pain treatment options can help place Disc Biacuplasty in that larger context.
When the disc is the pain generator
Discogenic pain often feels deep, central, and stubborn. Many patients describe pain that worsens with prolonged sitting, bending, or transitions from sitting to standing. It may not behave like classic sciatica. There may be no dramatic leg pain, numbness, or weakness. Instead, the disc itself acts like an irritated structure that keeps sending pain signals.
Clinical perspective: Disc Biacuplasty isn't a general fix for every form of back pain. It's a targeted treatment for a very specific pain pattern and anatomy.
That distinction matters. A treatment can be excellent and still be wrong for the wrong diagnosis.
Why patients find this option reassuring
Disc Biacuplasty appeals to people who are caught in the middle. They're beyond conservative care, yet they may not want, need, or qualify for a major surgical procedure such as fusion. The procedure is designed to treat the damaged disc from within, without an open incision. For the right person, that can feel less like “doing something drastic” and more like choosing a precise next step.
Understanding the Source of Discogenic Pain
A healthy spinal disc works like a resilient pressure cushion between the bones of the spine. It absorbs force when you sit, bend, walk, and lift. The outer ring of the disc, called the annulus fibrosus, is built to contain pressure while the inner portion helps distribute load.
A useful way to picture it is this. Think of a healthy disc like a new tire. The sidewall is intact, the internal pressure is balanced, and the structure handles road stress smoothly. A painful degenerative disc is more like a worn tire with internal fraying. It may still look present on imaging, but the outer fibers have weakened and tiny internal tears can become a persistent source of irritation.
Why this kind of pain is confusing
Many people assume all back pain comes from a disc “slipping” and pressing on a nerve. That's one pattern, but it isn't the only one. In discogenic pain, the problem may be the disc itself. Internal tears in the annulus can become inflamed, and pain-sensing nerve fibers can extend into areas where they shouldn't be. The result is a disc that hurts when loaded, compressed, or stressed.
This is why the pain can feel mechanical yet still remain chronic. The structure that's supposed to cushion movement has become sensitive to movement.
For some patients, advanced imaging helps clarify that difference. A high-quality evaluation, including MRI diagnostics in regenerative medicine, can help distinguish disc-related pain from other spinal sources.
Disc pain is not the same as facet pain
Readers often encounter mixed signals. Two nearby structures can produce very different problems.
Discogenic pain: Usually deeper and more central. It often worsens with sitting, bending, and sustained load.
Facet joint pain: Often behaves more like pain with extension, rotation, or joint compression.
Nerve compression pain: More likely to radiate down the leg in a clear nerve distribution.
A precise diagnosis changes the treatment path. Treating facet pain like disc pain, or disc pain like nerve compression, often leads to disappointment.
Why that distinction matters before any procedure
Disc Biacuplasty was developed for pain arising from the disc annulus. If the main pain source sits elsewhere, the procedure won't address the true problem. That's why thoughtful workup matters more than enthusiasm for any single treatment.
How Disc Biacuplasty Restores Function
Disc Biacuplasty uses the TransDiscal™ System, which places water-cooled radiofrequency probes bilaterally into the disc annulus. The procedure safely delivers energy to denervate the damaged disc and promote collagen repair, strengthening the tissue without incisions, as described in this overview of Disc Biacuplasty disc denervation.
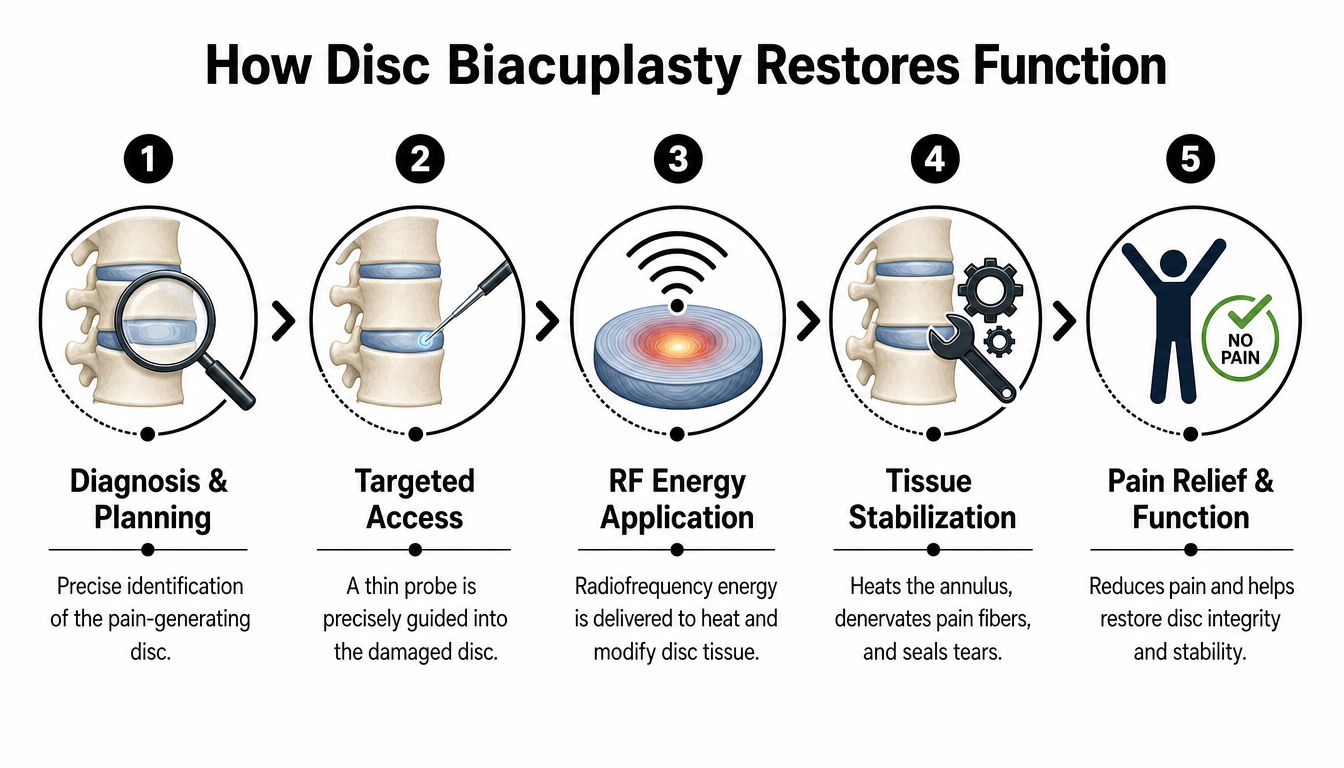
The phrase “radiofrequency” can sound more intimidating than the procedure is. In practical terms, clinicians guide specialized probes into the painful disc and apply controlled thermal energy in a way that targets the pain-producing tissue while protecting nearby structures. The water-cooling system helps shape that energy delivery with greater control.
Two jobs happening at once
The treatment is easier to understand if you think of it as doing two things at the same time.
Quieting pain fibers
The irritated nerve endings within the damaged annulus are treated with targeted heat. This is the “denervation” part. The goal is to reduce the disc's abnormal pain signaling.Supporting the disc wall
Controlled heating also affects collagen in the annulus. You can picture this as gently tightening and stabilizing frayed tissue, somewhat like warming and reshaping a stretched fabric so it holds together better.
That second piece matters because patients often assume the procedure only numbs pain. It's more accurate to say it treats a painful disc environment in a way that may also reinforce the damaged tissue.
For readers exploring adjacent non-surgical approaches, our guide to regenerative disc therapy explains where biologic strategies may fit into spine care.
What the probe placement actually means
The technical language can be hard to visualize, so here's the simplified version. The physician uses imaging guidance to approach the painful disc from both sides. The probes are positioned in the outer disc wall where annular pain tends to originate. Energy is then applied in a controlled pattern.
What patients often find reassuring: Disc Biacuplasty is designed to address the source of pain within the disc itself, not simply mask symptoms for a few days or weeks.
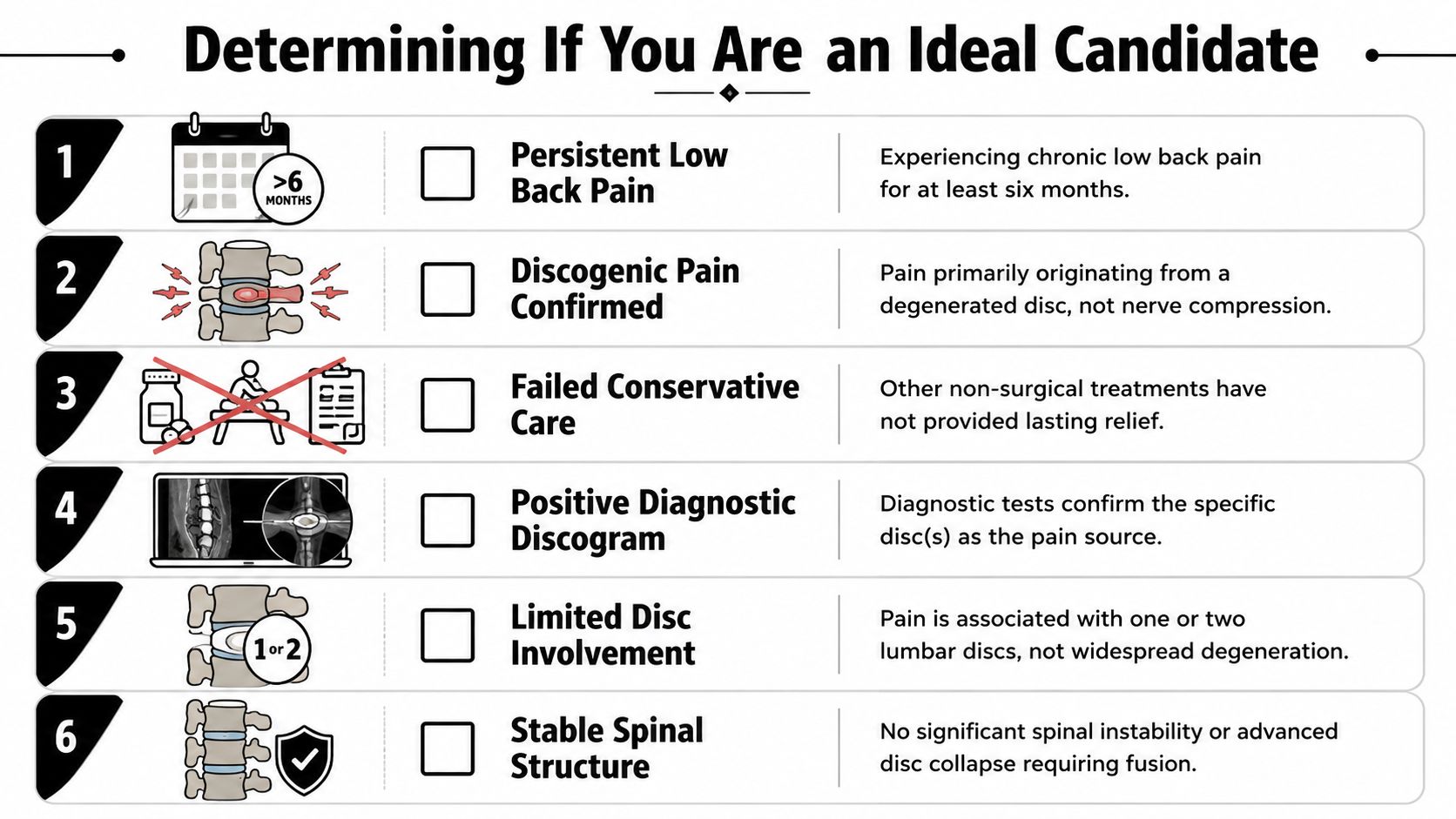
Determining If You Are an Ideal Candidate
The most important question isn't whether Disc Biacuplasty works in general. It's whether your spine problem matches the pattern it was designed to treat.
That requires more than a symptom checklist. A patient can have “disc degeneration” on an MRI and still have pain primarily coming from facet joints, instability, or another structure. Good candidate selection protects patients from the wrong procedure and gives the right patients a clearer path forward.
The profile that tends to fit best
Disc Biacuplasty is most effective for contained lumbar degenerative disc disease, and its efficacy is significantly lower when pain stems from high-grade facet degeneration or advanced disc disease, which highlights the need for precise imaging and patient selection, according to this review on candidate selection for biacuplasty.
In plain language, that usually points toward a patient with:
Persistent low back pain: The symptoms have stayed present despite thoughtful conservative care.
Contained disc pathology: The disc is damaged, but not in a pattern of major rupture requiring a very different strategy.
Reasonable structural preservation: The disc hasn't completely collapsed and the segment isn't clearly unstable.
Limited competing pain sources: Severe facet arthropathy can cloud the picture and reduce the chance of success.
What to ask about your MRI and exam
Patients often feel intimidated by radiology reports. You don't need to decode every line. You do need to know whether the findings fit a discogenic pain pattern.
Ask your physician questions like these:
Which disc is believed to be causing pain? A vague answer usually means the diagnosis isn't settled.
Are the facet joints relatively preserved? If not, the pain may not be primarily disc-driven.
Is the disc contained or severely disrupted? That distinction can change the treatment plan.
Is there significant instability or advanced collapse? If yes, a stabilizing surgery may become more relevant than an intradiscal procedure.
The strongest consultations happen when imaging, symptoms, and physical examination all point in the same direction.
Why some patients don't benefit
A common misconception is that a minimally invasive procedure is worth trying “just in case.” In spine care, that mindset can waste time and confuse the recovery picture.
Patients with advanced degeneration, major facet involvement, or pain patterns dominated by nerve compression often need a different path. Sometimes that means rehab and diagnostics. Sometimes it means a surgical opinion. Sometimes it means combining structural treatment with broader inflammation management.
At Longevity Medical Institute, one available option is COOLIEF® TransDiscal® Disc Biacuplasty, performed with real-time fluoroscopic guidance, in some cases alongside regenerative biologic therapies when clinically appropriate. That doesn't replace the need for careful selection. It makes selection even more important.
Your Treatment Journey from Procedure to Recovery
Most patients feel calmer once they understand the sequence. The experience is usually far more structured and less dramatic than they imagined.
The procedure is commonly performed as an outpatient treatment using local anesthesia with light sedation. That means you're comfortable, monitored, and not recovering from a large incision. Imaging guidance is used throughout to place the instruments accurately inside the targeted disc.
The day of the procedure
You'll typically arrive having already completed imaging review, clinical evaluation, and consent discussions. The treatment area is prepared in sterile fashion. The physician then guides the probes into the painful disc and performs the radiofrequency treatment.
Afterward, you spend a short period in observation before going home. The immediate period is generally not described as an instant transformation. It's more like the start of a healing phase. The disc has been treated, but tissues still need time to settle.
The first weeks after treatment
Recovery usually unfolds in stages rather than in a straight line. Some soreness early on isn't surprising. Patients are often guided toward activity modification, progressive walking, and a measured return to movement rather than aggressive exercise.
This is where rehab matters. Rest alone rarely rebuilds function. The spine responds best when the painful structure is treated and the surrounding movement patterns are retrained. That's why coordinated follow-up and advanced rehabilitation for pain relief and movement restoration can be such an important part of the process.
Healing after Disc Biacuplasty is less like flipping a light switch and more like turning down the alarm while rebuilding trust in movement.
What outcomes can look like
In a clinical trial of 15 patients with chronic discogenic low back pain, 57.1% reported at least a 50% decrease in pain, 78.6% experienced a reduction of two or more points on the Visual Analog Scale and a 10-point improvement in Oswestry Disability Index scores, 71.4% reported satisfaction, and no complications were observed at the 6-month follow-up, according to the published study on TransDiscal Biacuplasty outcomes.
A separate randomized study found clinical success in 30% of biacuplasty patients versus 3% in the sham group, with significantly greater improvements in physical functioning, pain ratings, and disability measures at 6 months. Among 29 patients originally randomized to biacuplasty, 22 (76%) were available for 12-month follow-up, and mean VAS scores improved from 6.7 to 4.4. Those findings are summarized in this medical policy review of percutaneous intradiscal radiofrequency biacuplasty.
Risks and realistic expectations
No spine procedure is risk-free, and good counseling should never pretend otherwise. The most useful framing is this: Disc Biacuplasty is minimally invasive, but it still requires skilled technique, proper diagnosis, and appropriate aftercare.
Reasonable expectations include:
Pain relief may be gradual: Some people improve steadily over weeks to months.
Function matters as much as pain: Sitting tolerance, walking, sleep, and confidence in movement are all meaningful markers.
Not every patient responds: A technically successful procedure can still underperform if the disc wasn't the true pain source.
Biacuplasty Compared to Other Spine Treatments
Patients usually aren't choosing between “nothing” and Disc Biacuplasty. They're choosing among several very different philosophies of care. Some options calm symptoms. Some alter mechanics. Some aim to stabilize or regenerate tissue. Some are reserved for structural failure that can't be managed less invasively.
That's why comparisons matter. The best treatment isn't the most advanced-sounding one. It's the one that matches the anatomy, pain source, and goals of the patient in front of you.
Comparison of Spine Treatment Options
| Treatment | Invasiveness | Mechanism | Best For |
|---|---|---|---|
| Conservative care such as physical therapy, medication, and activity modification | Low | Symptom control, movement retraining, load management | Early-stage pain, recovery support, patients still likely to improve without procedures |
| Epidural or other spine injections | Low to moderate | Reduces inflammation or helps diagnose a pain source | Flares, nerve-related pain, short-term diagnostic or therapeutic use |
| Disc Biacuplasty | Moderate, minimally invasive | Intradiscal radiofrequency treatment that denervates painful disc tissue and supports annular collagen repair | Carefully selected patients with contained discogenic low back pain |
| Allogeneic regenerative injections | Moderate, minimally invasive | Biologic support aimed at tissue environment and inflammation modulation | Selected orthopedic and spine cases where a regenerative strategy fits the diagnosis |
| Spinal fusion | High | Surgically stabilizes a painful or unstable spinal segment | Advanced structural disease, instability, or cases where less invasive care isn't appropriate |
Where Disc Biacuplasty fits
Disc Biacuplasty occupies a useful middle ground. It's more targeted than repeating generalized conservative care when that phase has already failed, yet it's far less invasive than fusion. For the right candidate, that's its value. It intervenes directly at the disc without moving immediately to a large surgical reconstruction.
It also differs from regenerative medicine. Biacuplasty uses thermal energy within the disc to treat discogenic pain and annular pathology. Regenerative approaches aim to influence the biologic environment in a different way. In practice, these aren't always competitors. They may address different problems or different layers of the same problem. Patients considering broader biologic care can compare options in our resource on regenerative medicine for back pain.
Some patients need symptom control. Some need mechanical stabilization. Some need surgery. Disc Biacuplasty sits between those lanes, and only works well when the diagnosis is exact.
The practical decision point
If your pain is clearly discogenic, structurally contained, and resistant to conservative care, Disc Biacuplasty may be a rational next step. If your spine shows advanced collapse, instability, or dominant facet disease, another route may make more sense.
That's why high-level spine care starts with matching the treatment to the pain generator, not with picking a favorite procedure.
Planning Your Treatment FAQs
How do I know if traveling for this procedure makes sense
Travel can make sense when you've already completed a meaningful amount of conservative care, your imaging is available for review, and you want a center that can combine diagnostics, procedure planning, and follow-up support in one coordinated process. For many patients, the decision comes down to confidence in diagnosis and logistics rather than geography alone.
Before making travel plans, gather your MRI reports, prior treatment history, medication list, and a short timeline of symptoms. That allows a consulting team to judge whether Disc Biacuplasty belongs in the discussion at all.
What does the consultation process look like for an international patient
Most patients do best with a staged review. First comes record collection and imaging review. Then comes a clinical consultation, often virtual at the outset, to decide whether your symptoms fit a discogenic pattern. If the case appears appropriate, the team can discuss travel timing, pre-procedure preparation, and the likely recovery window.
A thoughtful consultation should also include reasons not to proceed. That's a sign of good medicine, not a barrier.
Is Disc Biacuplasty covered by insurance
Coverage varies widely by plan, region, and the medical policies used by an insurer. Some patients pursue the procedure through self-pay pathways, while others seek reimbursement support using clinical documentation. The practical step is to verify benefits early and ask exactly what records are needed for preauthorization or claims review.
What is recovery like in San José del Cabo
Many patients appreciate recovering in a setting that supports quiet walking, hydration, comfortable accommodations, and a less stressful pace. The key isn't tourism. It's environment. Early recovery tends to go best when your schedule is protected and movement can resume gradually without the pressure of immediate long commutes or a rushed return to routine.
Can Disc Biacuplasty be combined with other treatments
Sometimes yes, but combination planning should be individualized. Some patients benefit from structured rehabilitation after the procedure. Others may also be evaluated for complementary regenerative strategies depending on the broader spine picture. The sequence matters, and the diagnosis still comes first.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: July 6, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.
If you'd like help understanding whether your MRI, symptoms, and prior treatment history fit a true discogenic pain pattern, Longevity Medical Institute offers consultation and treatment planning through its educational resource hub at Treatments & Resources.