Regenerative Disc Therapy: Modern Solutions for Back Pain
Back pain often begins subtly. A long commute becomes uncomfortable, golf feels tighter after nine holes, or bending to tie your shoes suddenly feels risky. In many people, the pain generator isn't just muscle tension. It may be the disc itself.
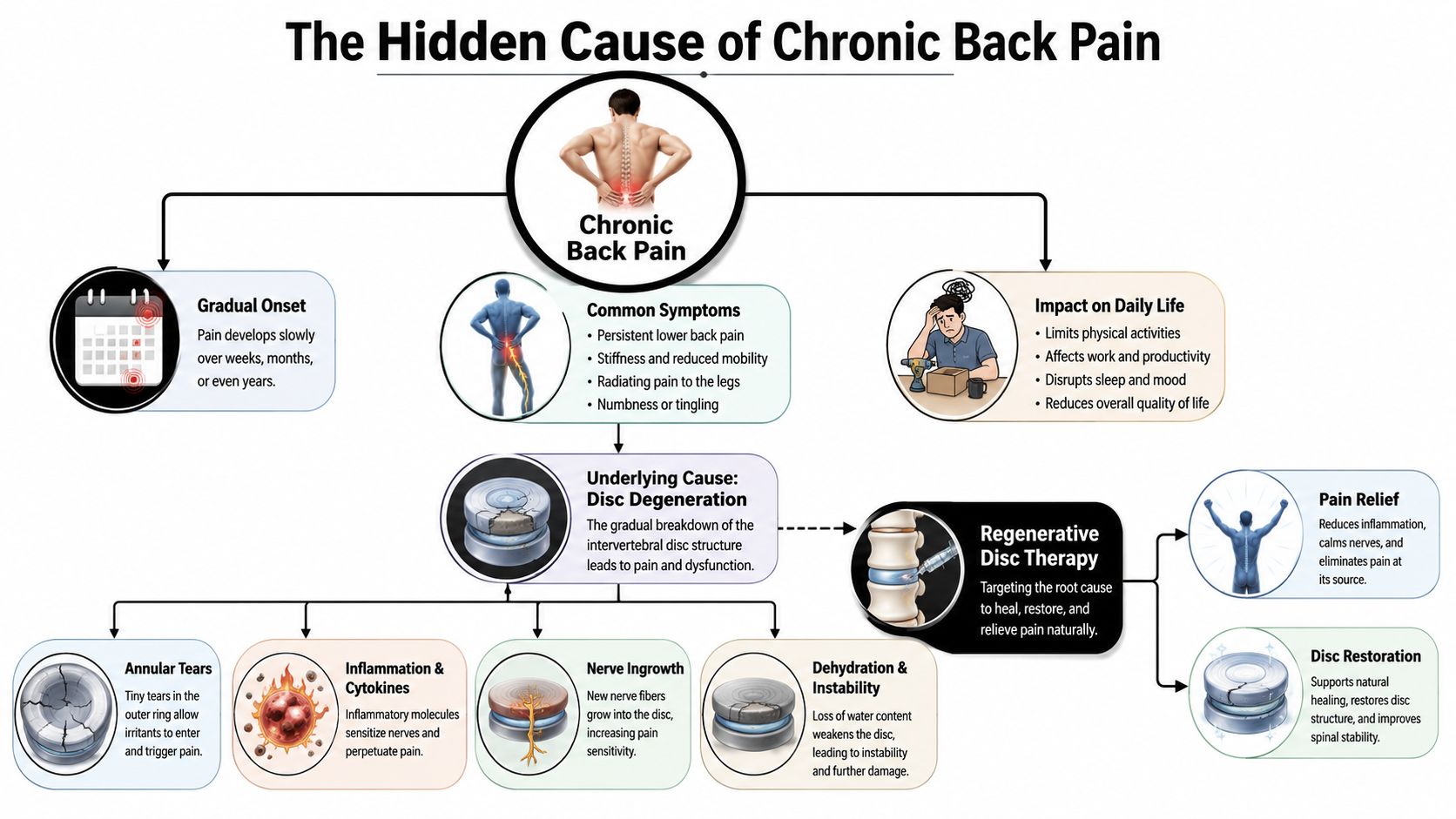
The Hidden Cause of Chronic Back Pain
A healthy spinal disc works like a pressure cushion between two vertebrae. The nucleus pulposus is the softer center, built to distribute load. The annulus fibrosus is the outer ring, made of layered fibers that contain the nucleus. The endplates sit above and below the disc and help with nutrient exchange.
That anatomy matters because discs heal slowly. Unlike muscle, a disc has a poor direct blood supply, so it doesn't receive the same steady delivery of oxygen and repair cells that other tissues do. A strained muscle can often calm down with rest, time, and movement. A damaged disc can stay irritated much longer.
Why a disc becomes painful
People often hear the phrase degenerative disc disease treatment and assume the disc is “worn out.” That's incomplete. A painful disc usually involves a mix of structural irritation and chemical inflammation.
Common drivers include:
Annular tears: Small disruptions in the outer ring can become pain generators.
Inflammation: The disc environment may release inflammatory cytokines that sensitize local tissue.
Nerve ingrowth: Nerves can grow into areas of the disc where they normally don't contribute much sensation.
Dehydration: The disc may lose water content and shock-absorbing capacity.
Instability: Even subtle abnormal movement can keep the area irritated.
Many patients often experience confusion regarding this matter. An MRI can show disc degeneration in someone with very little pain. Another patient can have intense discogenic low back pain with imaging that looks only moderately abnormal. The scan is helpful, but the diagnosis comes from matching symptoms, physical exam, and imaging together.
In Plain Terms
A disc can look bad and not hurt. A disc can also look only mildly changed and hurt a lot. The key question is whether that disc is actually the pain generator.
The disc is not the only possible culprit
Low back pain isn't one condition. It's a region of the body with several possible pain sources.
Here's a simple comparison:
| Pain source | Typical pattern | What patients often notice |
|---|---|---|
| Disc pain | Deep, central low back pain, worse with sitting, bending, coughing, or prolonged driving | “It feels like pressure deep inside my spine.” |
| Facet joint pain | More local pain off to one side, worse with standing back up or extending the spine | “Leaning backward pinches.” |
| SI joint pain | Often lower and more one-sided, can refer into buttock or groin | “It feels low, almost below the belt line.” |
| Muscle strain | Tender, tight, activity-related pain | “It grabs or spasms.” |
| Nerve compression | Back pain with leg pain, numbness, tingling, or weakness | “The pain shoots down my leg.” |
| Spinal stenosis | Pain or heaviness with walking or standing, relieved by leaning forward | “The cart at the grocery store helps.” |
Disc pain often flares with sitting, because sitting can increase disc pressure. That's why people with lumbar disc pain may tolerate walking better than desk work or long drives.
What regenerative disc therapy means
Regenerative Disc Therapy refers to a strategy that aims to address disc-related pain while preserving the native disc rather than removing it. In this guide, I'm focusing on a specific combination: COOLIEF® TransDiscal® Disc Biacuplasty paired with biologics such as PRP, allogeneic stem cells, and exosomes.
The idea is straightforward:
Reduce pain signaling coming from the painful outer disc.
Improve the disc environment by addressing inflammation and supporting repair signaling.
Protect function so the patient can move, rehabilitate, and recover more effectively.
This is not a promise of a brand-new spine. It's a minimally invasive attempt to help the disc become less painful and more biologically stable.
For people exploring broader options in regenerative medicine for back pain, this distinction matters. The goal is often better pain control, better function, and disc preservation, not fantasy-level structural reversal.
Why daily life slowly exposes disc problems
Disc pain rarely begins with one dramatic event. More often, it builds from repetition. Hours of sitting, years of lifting, rotation during sports, vibration from driving, and deconditioning all add up. Then one small movement becomes the moment you finally notice it.
A common story sounds like this:
Sitting through work becomes harder.
The back starts aching after driving.
Golf swings feel restricted.
Lifting a grandchild causes a sharp reminder.
Bending over the sink or tying shoes becomes the day's most uncomfortable moment.
That pattern matters because it suggests a load-sensitive structure. The disc often behaves that way.
A painful disc usually announces itself during ordinary life before it shows itself dramatically.
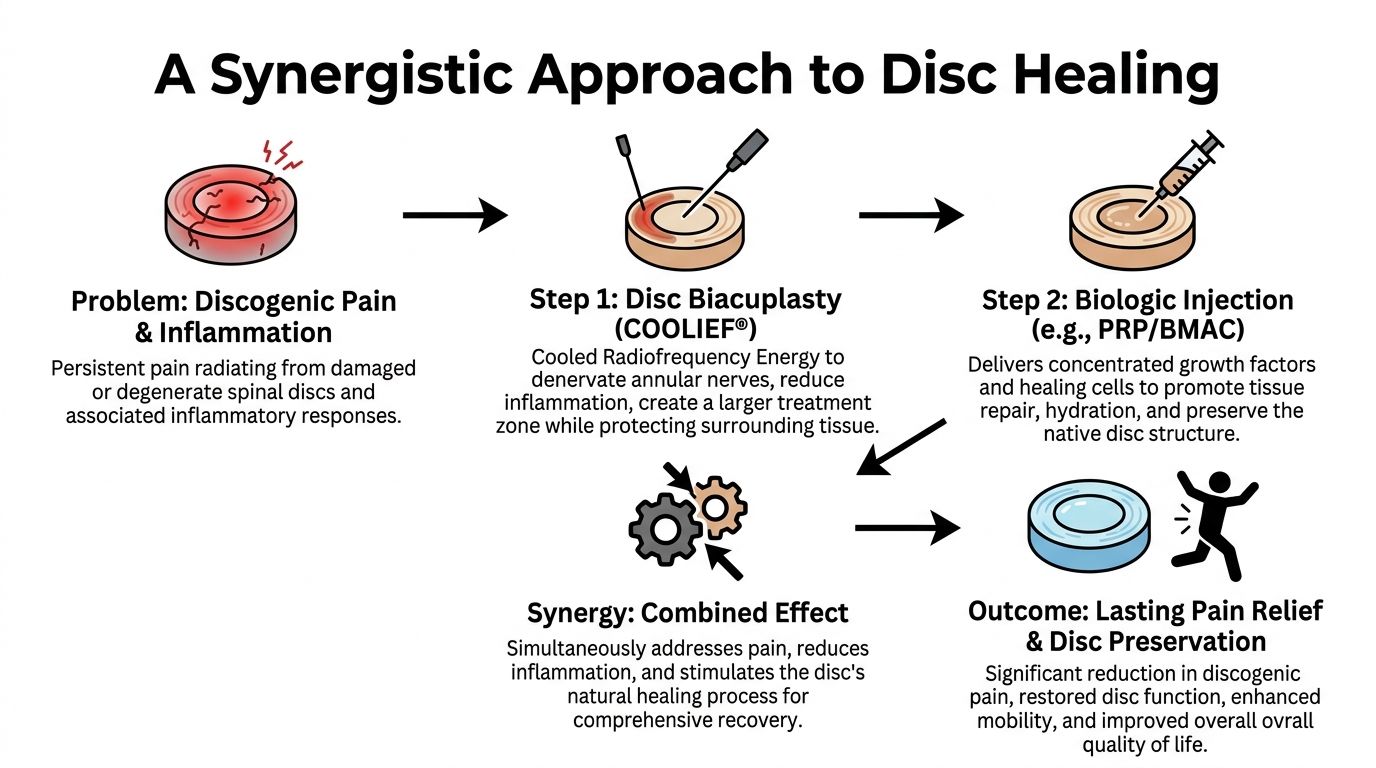
A Synergistic Approach to Disc Healing
When a disc is painful, one intervention may not address the whole problem. Pain signaling, local inflammation, and a poor healing environment can exist at the same time. That's why combining Disc Biacuplasty with biologics is attracting interest in regenerative medicine for back pain.
What COOLIEF TransDiscal Disc Biacuplasty does
COOLIEF® TransDiscal® Disc Biacuplasty is an intradiscal therapy that uses cooled radiofrequency energy to treat pain arising from the outer annulus. Under imaging guidance, specially placed probes target the painful posterior annulus. The treatment is designed to create controlled heating in the annular tissue.
The cooling feature sounds counterintuitive, but it serves a purpose. Cooling the probe helps create a larger treatment zone while protecting adjacent tissue at the probe interface. In plain terms, that means the system can distribute therapeutic heat in a controlled way rather than just overheating a tiny point.
The painful annulus can house irritated nerve fibers. By reducing pain signaling in that region, Disc Biacuplasty may lower the disc's ability to keep triggering chronic pain. It doesn't remove the disc. It doesn't fuse the spine. It aims to treat a specific pain mechanism while preserving native structure.
Why biologics are added
After pain signaling is addressed mechanically and thermally, biologics may help support the disc environment. That's the rationale behind adding PRP, allogeneic mesenchymal stem cells, and exosomes in carefully selected cases.
A simple analogy helps. If Biacuplasty is like turning down the alarm system, biologics may help calm the irritated neighborhood around it.
Later in the section, I'll separate what's supported by stronger evidence from what remains emerging. First, it helps to understand what each biologic is meant to do.
PRP and the signaling role of platelets
PRP for disc degeneration refers to platelet-rich plasma, a concentration of platelets that contains growth factors and signaling molecules. PRP isn't a structural implant. It's a biochemical signal source.
In disc care, PRP is used with the idea that it may:
Modulate inflammation: It may help shift the local environment away from persistent irritation.
Support tissue signaling: Growth factors may encourage repair-oriented cellular activity.
Assist remodeling: In some patients, this may support a healthier healing response.
PRP is appealing because it's conceptually simple. It's not expected to regrow an entire damaged disc. It may help the disc environment behave less like an inflamed wound and more like a healing tissue.
Mesenchymal stem cells and what they likely do
When people hear stem cells for degenerative disc disease, they often imagine the cells turning into a brand-new disc. That's not how I counsel patients. The more realistic discussion is about paracrine signaling, immunomodulation, and support for repair processes.
At our center, we use allogeneic cell sources rather than autologous approaches. Our biotechnology lab produces five different stem cell types, including placental, Wharton's jelly, adipose, endometrial, and dental pulp.
The clinical theory behind intradiscal stem cell use includes:
| Potential role | What that means in practice |
|---|---|
| Paracrine signaling | Cells release signals that may influence surrounding tissue behavior |
| Immunomodulation | They may help calm excessive inflammatory signaling |
| Repair support | They may support matrix maintenance and tissue remodeling |
| Microenvironment support | They may help the disc become less hostile to recovery |
A broader review of stem cell therapy for degenerative disc disease reported that mesenchymal stem cell injections can yield an 85% reduction in pain within the first three months, with improved disc hydration seen as increased T2 MRI signals, while also noting that published trials have not consistently demonstrated reliable structural repair of annular tears or nucleus pulposus reconstitution and that the therapy remains investigational rather than FDA-approved specifically for intervertebral disc repair in routine care (peer-reviewed review on stem cell therapy for degenerative disc disease).
That distinction is essential. Pain relief can be meaningful even when full structural restoration isn't predictable.
Exosomes and extracellular signaling
Exosomes for back pain are even more emerging. Exosomes are small extracellular vesicles that carry signaling molecules between cells. They don't replace tissue directly. Their proposed value lies in cell-to-cell communication, anti-inflammatory signaling, and support for tissue repair pathways.
The theory is attractive because discs are biologically difficult places to heal. They're low-oxygen, low-nutrient environments. Any therapy that helps coordinate a more constructive local response is worth scientific attention. Still, this remains an area where clinical enthusiasm has outpaced definitive long-term evidence.
Why the combination may make sense
Combining COOLIEF TransDiscal, PRP, stem cells, and exosomes is based on a layered strategy rather than a single magic mechanism.
Biacuplasty addresses pain signaling.
PRP may add concentrated growth-factor signaling.
Stem cells may support immunomodulation and repair-oriented paracrine effects.
Exosomes may contribute extracellular communication that supports tissue recovery.
Science Beneath
A painful disc often has both a mechanical problem and a biological problem. A combined approach tries to address both.
That said, the combination itself is promising but still evolving. We have rationale. We have related evidence for individual components. We also have a responsibility to separate established outcomes from theory. In some patients, a combined plan may be reasonable. In others, a simpler or different strategy makes more sense.
Some patients also ask whether other supportive tools such as hyperbaric oxygen therapy and stem cells might complement regenerative programs. Those conversations depend on diagnosis, overall goals, and whether the added therapy fits the biology of the case.
Your Procedure Day What to Expect
Most patients feel better once they know the sequence. Uncertainty creates anxiety. A clear plan makes the experience more manageable.
Before the procedure
The process starts with a consultation, a physical examination, and imaging review. MRI findings matter, but they're interpreted alongside your symptoms and functional pattern. The main question is whether the suspected disc matches the pain story.
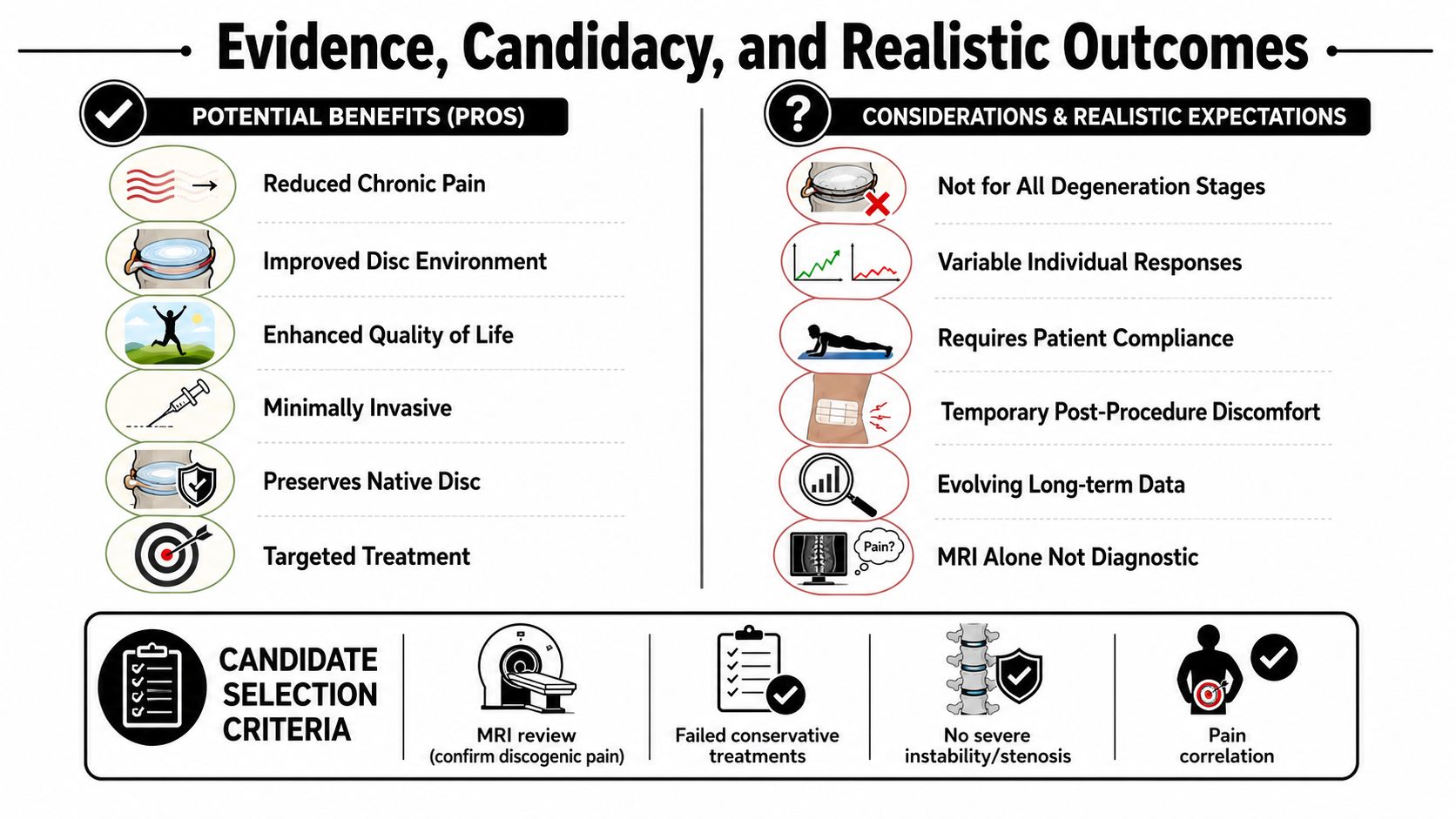
Candidate selection usually focuses on:
Chronic discogenic pain
Contained disc damage
Mild-to-moderate degeneration
Failure of appropriate conservative care
No clear surgical red flags
Advanced imaging often helps narrow the target and rule out competing pain generators. That's one reason patients sometimes undergo detailed review through resources such as MRI diagnostics in regenerative medicine in Los Cabos.
Who is involved in the procedure
This is a physician-led, image-guided procedure. It's not a one-person event.
Your team may include:
| Team member | Role |
|---|---|
| Primary physician | Performs or administers the procedure and makes real-time treatment decisions |
| Assisting physician | Supports needle placement, workflow, and procedural precision |
| Nurse | Monitors you, helps with preparation, recovery, and discharge instructions |
| Anesthesiologist | Provides sedation and comfort support when used |
| Radiology professional | Operates the C-arm for real-time fluoroscopic guidance |
This team-based approach is about precision, comfort, and safety. Disc procedures require accurate placement. Real-time imaging helps confirm trajectory and depth.
During the treatment
After preparation and positioning, the skin is cleaned and the treatment area is draped in sterile fashion. Sedation may be used depending on the treatment plan and patient needs. The physician uses C-arm fluoroscopy to guide needle and probe placement into the intended disc level.
The Biacuplasty portion targets the painful annulus with controlled cooled radiofrequency treatment. Once that step is completed, the physician may place the planned biologic into the disc under imaging guidance.
The sequence typically follows this logic:
Confirm target level
Position needles and probes under fluoroscopy
Perform Disc Biacuplasty
Deliver biologic injection
Monitor in recovery
Discharge with activity restrictions
Patients are usually discharged the same day after observation and instructions.
The procedure is minimally invasive, but the disc still needs time to calm down and remodel afterward.
After discharge
You'll usually go home with guidelines about walking, sitting limits, lifting restrictions, and when to call the doctor. Some soreness is expected. You should arrange a ride home if sedation is used.
A smooth procedure day doesn't mean instant results. The treatment aims to start a process. The disc doesn't heal on the clinic schedule. It heals on a biological timeline.
Evidence Candidacy and Realistic Outcomes
Patients deserve a clear separation between what's established, what's encouraging, and what's still uncertain. That's especially true in Regenerative Disc Therapy.
What the evidence suggests
Disc Biacuplasty has clinical use as a minimally invasive option for selected patients with discogenic pain, particularly when the goal is disc preservation rather than surgery. The mechanism is coherent, patient selection is critical, and outcomes appear to depend heavily on choosing the right pain generator.
PRP has biologic plausibility for intradiscal use because it concentrates signaling molecules and growth factors. The limitation is that outcomes aren't uniform, and technique, patient selection, and disc condition likely matter a great deal.
Stem cell-based intradiscal therapies have generated some of the most interesting data in the field. In a Phase II FDA-allowed study on Discogenic Progenitor Cell Therapy, the high-dose group achieved a 62.79% reduction in low back pain at 52 weeks, had a 100% safety rate regarding serious complications in the active group, and showed a statistically significant increase in disc volume at the two-year mark, suggesting structural regeneration in that specific investigational setting (Phase II FDA-allowed Discogenic Progenitor Cell Therapy report).
That's encouraging. It's not the same as saying every stem cell protocol, every clinic, or every disc condition will produce the same outcome.
Exosomes are biologically interesting and clinically discussed, but the evidence base is less mature for intradiscal applications. They belong in the category of emerging science rather than settled standard of care.
Good candidates and poor candidates
The best candidate is not only a person with back pain and a disc abnormality on MRI. The best candidate is someone whose clinical story, examination, imaging, and failure of conservative treatment all line up.
A reasonable candidate often has:
Chronic discogenic low back pain
Contained disc damage
Mild-to-moderate disc degeneration
Symptoms that correlate with MRI findings
Persistent pain despite conservative care
A poor candidate often has one of the following:
Severe instability
Severe spinal stenosis
Progressive neurologic deficit
Active infection
Tumor
Fracture
Cauda equina symptoms
A condition that clearly requires surgery
For patients researching biologic options further, this candidacy discussion overlaps with what's covered in stem cell therapy for spinal disc degeneration.
Potential benefits and realistic expectations
Realistic goals are functional. A successful outcome may include:
| Potential benefit | What it can mean day to day |
|---|---|
| Less pain | Easier sitting, driving, or standing |
| Better mobility | Less guarding during ordinary movement |
| Improved endurance | More walking tolerance and better activity recovery |
| Medication reduction | Less reliance on pain medication for some patients |
| Better quality of life | More confidence with work, travel, and family activities |
| Possible surgery delay | A chance to postpone or avoid more invasive treatment in selected cases |
Risks and limitations
Every intradiscal procedure has risks. These should be discussed plainly, not hidden behind optimism.
Potential risks include:
Infection
Bleeding
Temporary soreness
Nerve irritation
Disc injury
Lack of improvement
Need for future surgery
Practical rule
The more honestly you understand the limits of a procedure, the better you're prepared to judge whether it's right for you.
A responsible discussion also includes uncertainty. The combination of Biacuplasty with PRP, stem cells, and exosomes is not a miracle cure. It's a strategy built from procedural science, regenerative logic, evolving evidence, and clinical judgment.
Navigating Your Recovery Journey
Recovery after Regenerative Disc Therapy usually feels more like a gradual climb than a sudden switch. Some patients improve in stages. Others feel a temporary flare before the trend turns in the right direction.
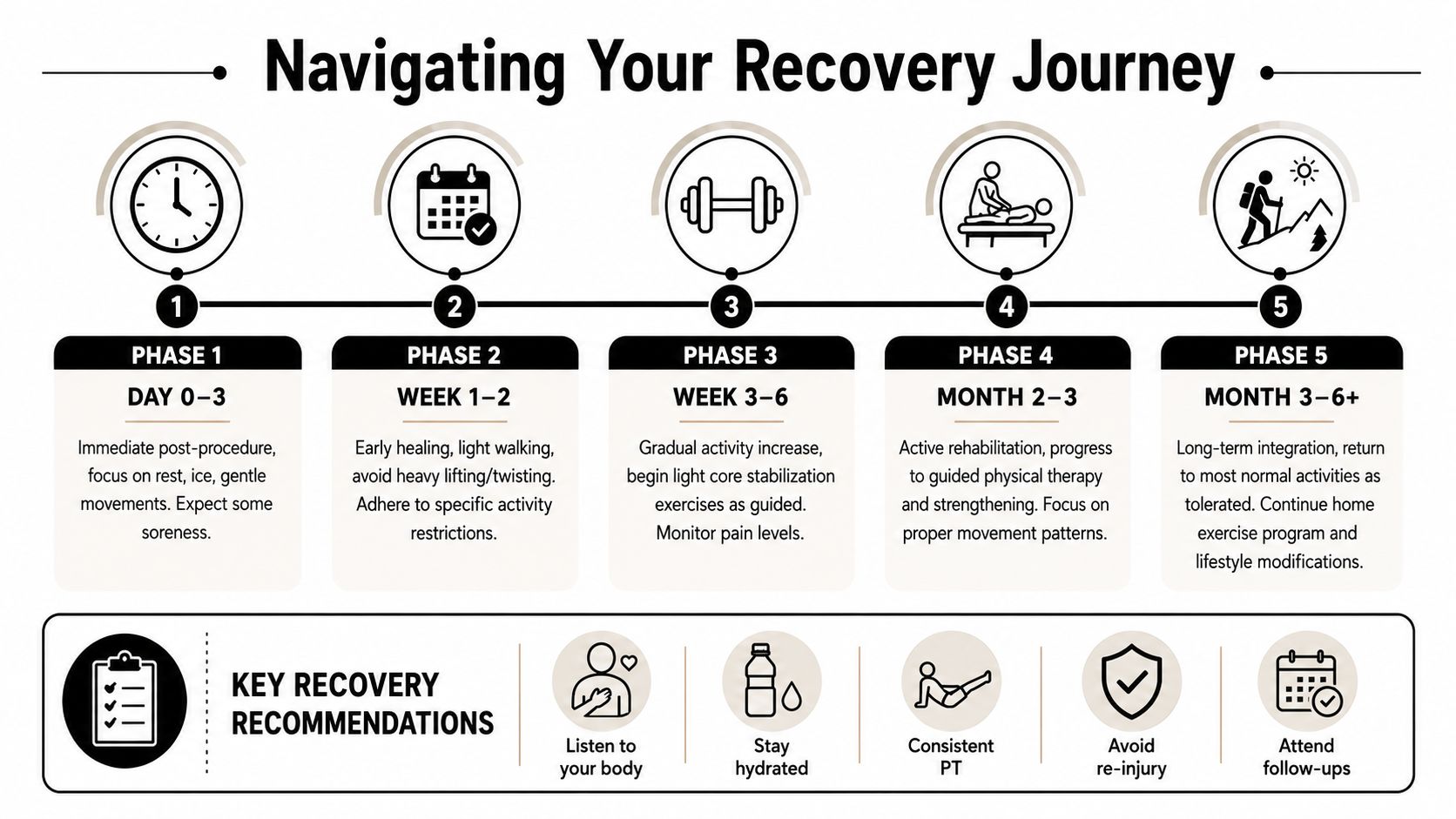
The general timeline
Here's the typical framework I use when counseling patients:
Days 1 to 7: Expect soreness, stiffness, and a need for relative rest. Short walks are usually appropriate.
Weeks 2 to 4: Symptoms often begin to stabilize. Walking generally increases as tolerated.
Weeks 4 to 8: Many patients start noticing early functional improvement.
Months 2 to 3: Pain and activity gains often become more noticeable.
Months 3 to 6: Healing and remodeling continue.
A patient who feels “not much yet” at the very beginning hasn't necessarily failed treatment. That's one of the biggest emotional traps in recovery.
Pain before progress
It is critical for patients to understand that benefits typically begin 4–12 weeks post-injection, with maximum effect often seen at 3–6 months. A common, temporary increase in pain for several days post-procedure is considered a normal reaction as the disc responds to the injection process (patient education on regenerative medicine timing and post-injection soreness).
That early discomfort can feel discouraging. The disc is a sensitive structure, and even a precisely performed injection can temporarily stir it up.
Early soreness doesn't automatically mean the procedure failed. It often means the disc noticed the intervention.
Healing is not linear
One of the hardest parts of recovery is variability. You may have a strong day followed by a frustrating day. That doesn't always mean you've gone backward.
A more useful way to judge progress is to ask:
Are flare-ups becoming less intense?
Is sitting tolerance improving over time?
Can I walk farther this week than last week?
Am I recovering faster after activity?
This week-to-week view is far more accurate than obsessing over one bad afternoon.
What helps the process
The patients who usually recover most successfully tend to follow simple but important habits:
| Helpful behavior | Why it matters |
|---|---|
| Short frequent walks | Encourages circulation and reduces stiffness |
| Respecting restrictions | Protects the treated disc from overload |
| Staying hydrated | Supports overall tissue recovery |
| Keeping follow-ups | Lets your clinician adjust the plan |
| Starting rehab at the right time | Builds support without irritating the disc |
If you want a broader sense of how biologic treatments often unfold after injection, recovery time after stem cell injection can help frame the pace, though disc recovery remains its own category.
Protecting Your Investment in Healing
The procedure is only one piece of the outcome. The months after treatment matter just as much. If the disc is trying to calm down and remodel, your daily habits either help that process or interfere with it.
Activity restrictions that matter
Early on, the disc doesn't like sudden load, repeated flexion, or aggressive rotation. That means you should avoid activities that combine bending, twisting, and lifting, especially under speed or fatigue.
Common restrictions include avoiding:
Prolonged sitting
Heavy exercise
Running and jumping
Golf, tennis, and pickleball
CrossFit
Deadlifts and weighted squats
Aggressive stretching
Chiropractic manipulation
Long-distance travel until cleared
These aren't arbitrary rules. They're ways to protect a healing disc from repeated mechanical stress.
Sitting, driving, and travel
Sitting loads the lumbar discs in ways many patients underestimate. During recovery, long seated periods often provoke symptoms faster than walking.
Use these practical strategies:
Limit sitting time: Change position regularly.
Use lumbar support: A small support roll can reduce strain.
Avoid long drives early: If unavoidable, stop and walk.
Recline when possible: Slight recline can be easier than upright sitting.
Get help with luggage: Lifting and twisting is a poor combination.
On flights, stand and walk every 30–60 minutes when allowed: Movement usually helps.
Walking, sleep, and basic recovery habits
Walking is one of the safest ways to restore confidence and circulation after an intradiscal procedure. Start small. Add time gradually. If symptoms flare, reduce the dose and resume more slowly.
A simple walking program often looks like this:
Begin with short, comfortable walks
Repeat them consistently
Increase duration before speed
Back off if the disc becomes more reactive
Build steadiness before adding exercise
Sleep position can also make a real difference. Most patients do best with back sleeping and a pillow under the knees or side sleeping with a pillow between the knees. Avoid stomach sleeping early if it increases lumbar extension or morning stiffness.
Nutrition, hydration, and nicotine
Discs don't heal because of one smoothie or one supplement. Still, the body heals better when the basics are handled well.
Focus on:
| Supportive habit | Why it helps |
|---|---|
| Protein intake | Provides building blocks for repair |
| Hydration | Supports general tissue function |
| Fruits and vegetables | Helps overall recovery and inflammatory balance |
| Whole foods | Reduces reliance on ultra-processed convenience foods |
| Omega-3-rich foods | Supports a healthier inflammatory profile |
| Limiting excessive alcohol | Helps protect recovery quality and sleep |
Nicotine deserves special emphasis. Smoking and nicotine reduce blood flow and oxygen delivery, and that may slow spinal tissue healing. For a structure that already heals poorly, this matters.
Rehabilitation is not optional
Biologics don't replace rehab. A calmer disc still needs a more capable body around it.
Rehabilitation often includes:
Walking progression
Core strengthening
Physical therapy
Posture work
Proper lifting mechanics
Sleep improvement
Weight management when relevant
One option patients consider for integrated diagnostics, procedure planning, and follow-up is Longevity Medical Institute, where image-guided regenerative spine care is paired with rehabilitation planning and broader regenerative services such as Stem Cell Therapy, Exosome Therapy, PRP Therapy, Cellular Regeneration Therapy, Conditions Treated, and Book Consultation.
Long-term success usually belongs to patients who respect the timeline, protect the disc, and build better support around it.
Frequently Asked Questions and Common Myths
Some conditions still need surgery. If you have a large herniation, instability, progressive weakness, cauda equina syndrome, tumor, infection, fracture, or severe stenosis, a regenerative approach may not be the right primary treatment. Safety comes first.
Frequently asked questions
Does this regrow the disc
Not in the way commonly imagined. A critical misconception is that stem cell therapy will fully restore disc height. Success is measured more by pain resolution and functional improvement than by a dramatic “growth back” on MRI, and expecting reversal of years of degeneration is scientifically unfounded.
How painful is the procedure
Most patients are more comfortable than they expect because the procedure is image-guided and sedation is used. Afterward, soreness is common. The disc can feel irritated before it settles.
How long is recovery
Recovery is gradual. Many patients move through early soreness, then stabilization, then progressive functional improvement over weeks to months. Full assessment takes patience.
When can I drive
You shouldn't drive the day of the procedure if you've had sedation. After that, driving depends on comfort, reaction time, medication use, and physician clearance. Short trips usually return before long commutes.
When can I fly
That depends on how recently you were treated, how long the flight is, and how reactive your back is with sitting. If you do fly, use lumbar support, avoid heavy luggage, and stand when allowed.
Can multiple discs be treated
Sometimes, yes. But more treatment isn't automatically better. The key issue is identifying the true pain generator or generators.
Can it be repeated
In some cases, repeat treatment may be considered. That depends on response, diagnosis, disc condition, and the reason symptoms returned.
How long do results last
There's no one answer. Durability depends on diagnosis, disc biology, activity habits, rehabilitation, and whether the treated disc was the main source of pain.
When should I call the doctor
Call promptly for fever, worsening neurologic symptoms, loss of bowel or bladder control, severe increasing pain that feels out of proportion, new weakness, or signs of infection.
Will I need physical therapy if I feel better
Usually yes. Pain relief without movement retraining often leads people back into the same mechanical patterns that irritated the disc in the first place.
Myths vs facts
| Myth | Fact |
|---|---|
| Myth 1. All back pain comes from muscles. | Many patients have discogenic pain, facet pain, SI pain, or nerve-related pain. |
| Myth 2. If MRI shows degeneration, that must be the pain source. | Imaging alone doesn't identify the true pain generator. |
| Myth 3. Regenerative Disc Therapy is the same as surgery. | It's a minimally invasive, disc-preserving strategy, not a fusion or disc replacement. |
| Myth 4. Biacuplasty burns the whole disc. | It uses controlled cooled radiofrequency to target a treatment zone in the painful annulus. |
| Myth 5. Stem cells create a brand-new disc. | The more realistic goal is signaling support, inflammation modulation, and functional improvement. |
| Myth 6. PRP is just a pain shot. | PRP is used for biologic signaling, not simple temporary numbing. |
| Myth 7. Exosomes directly rebuild tissue on command. | Exosomes are signaling vesicles with emerging applications, not guaranteed structural rebuilders. |
| Myth 8. If I'm sore after treatment, it failed. | Temporary post-procedure soreness can be normal. |
| Myth 9. Relief should be immediate. | Disc healing often unfolds gradually. |
| Myth 10. Once pain improves, restrictions no longer matter. | Early overloading can aggravate a healing disc. |
| Myth 11. Walking is bad for a healing disc. | Gentle walking is often one of the safest recovery tools. |
| Myth 12. Bed rest is the fastest way to recover. | Excessive rest often increases stiffness and deconditioning. |
| Myth 13. Chiropractic manipulation is always safe right after treatment. | Aggressive manipulation is often restricted early in recovery. |
| Myth 14. If one disc is abnormal, every abnormal disc should be injected. | The target should match the clinical pain pattern. |
| Myth 15. Good candidates are simply people who want to avoid surgery. | Good candidacy depends on diagnosis, imaging correlation, and the absence of surgical red flags. |
The best outcomes usually start with the most accurate diagnosis, not the most aggressive treatment.
Final Thoughts From Dr Sanford
When I speak with patients about Regenerative Disc Therapy, I try to give them two things at once. I want them to feel hopeful, and I want them to understand the limits clearly. Both matter.
A painful disc can be stubborn. It sits deep in the spine, heals slowly, and often affects life in quiet but relentless ways. Sitting becomes strategic. Travel becomes tiring. Exercise becomes uncertain. That's why a careful, minimally invasive approach can be so valuable when the diagnosis is right.
My view is simple. Precise diagnosis comes first. Patient selection comes next. Procedure choice comes after that. COOLIEF® TransDiscal® Disc Biacuplasty, combined with PRP, allogeneic stem cells, and exosomes, represents a thoughtful attempt to reduce pain signaling while supporting a healthier disc environment. In the right patient, that may improve pain, function, and daily confidence.
It's still important to say what this therapy is not. It's not a miracle cure. It doesn't guarantee complete structural reversal. It doesn't replace rehabilitation, sleep, nutrition, movement retraining, or good judgment during recovery.
The most successful patients usually approach treatment as a partnership. They understand why the disc hurts. They respect restrictions. They commit to rehabilitation. They focus on functional progress, not fantasy imaging goals.
If you're considering this path, ask careful questions. Make sure your symptoms, exam, and imaging line up. Ask what's proven, what's emerging, what's clinical experience, and what remains theory. That level of clarity protects you.
When the diagnosis is sound and expectations are realistic, modern regenerative spine care can be a meaningful step toward getting your life back.
If you'd like help determining whether a physician-led, image-guided regenerative spine approach fits your case, schedule a consultation with Longevity Medical Institute. We publish patient education and treatment resources at Treatments & Resources.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: July 5, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.