Stem Cell Therapy for Parkinson’s Disease
Parkinson's disease changes ordinary moments first. A shirt button takes longer. A fork feels less steady. A walk across the room requires more intention than it once did. For many people, the hardest part isn't only the movement itself. It's the uncertainty of what comes next, and the flood of headlines promising breakthroughs that are difficult to interpret.
That's where stem cell therapy enters the conversation. Not as a miracle claim, and not as an approved cure, but as one of the most advanced areas of modern regenerative science. In Parkinson's disease, researchers are studying whether carefully prepared cells might help address one of the condition's central biological problems: the loss of dopamine-producing neurons.
For a discerning patient, the right question isn't, “Does stem cell therapy work?” The better question is, “Which type of stem cell strategy are we talking about, what is it designed to do, and what stage of evidence supports it?” Those distinctions matter. They separate rigorous clinical science from vague marketing, and they help patients make decisions from a place of clarity rather than urgency.
A New Horizon for Parkinson's Wellness
A patient sits across from me and asks a fair, difficult question: “Are stem cells a real option for Parkinson's, or another headline I should be wary of?” The honest answer requires both hope and restraint.
Parkinson's disease places people in a hard position. Daily life demands practical decisions about symptoms, medication timing, sleep, energy, and function. At the same time, research news keeps pointing toward a more restorative future. Stem cell science matters in that space because it is testing whether medicine can do more than compensate for lost function. It is examining whether carefully prepared cells might one day help repair part of the underlying biological problem.
That possibility is real enough to study seriously. It is not ready to be described as standard care. In Parkinson's disease, stem cell treatment remains investigational, with the strongest work taking place in regulated clinical trials under close follow-up.
Patients often hear the phrase “stem cell therapy” and picture one general treatment. However, the approach is much more precise. In Parkinson's research, scientists are not testing a vague wellness intervention. They are studying specific cell products, specific delivery methods, and specific goals inside the brain. A useful comparison is an orchestra. If one section has gone quiet, the answer is not to add random sound. The answer is to introduce the right players, in the right place, at the right time, under careful direction.
That is why this moment deserves attention. The field has progressed from broad theoretical promise to tightly designed human studies that ask concrete clinical questions. Can the cells be manufactured consistently? Can they be delivered safely? Can they survive where they are placed? Can they function in a way that is biologically meaningful? Those are the questions that separate serious translational medicine from promotional language.
For a patient evaluating options, the practical lesson is simple. Ask what is being tested, why those cells were chosen, how they are administered, and whether the treatment is part of a legitimate trial or an unregulated commercial offering. The more specific the answers, the more credible the conversation.
At Longevity Medical Institute, our philosophy is aligned with that standard of care. We focus on safety, physiology, and cellular orchestration. In other words, the body performs best when signals, immune balance, tissue support, and repair mechanisms are working in concert. Our broader framework for how stem cell therapy works in regenerative medicine reflects that principle. For Parkinson's disease specifically, any cell-based treatment aimed at replacing or restoring dopamine-related function should be understood as investigational unless offered within an appropriate regulatory pathway.
Clarity protects patients. It also preserves room for justified optimism. The goal is not to dismiss innovation. The goal is to understand where the science stands, and what responsible care looks like while that science continues to mature.
Understanding Parkinson's at the Cellular Level
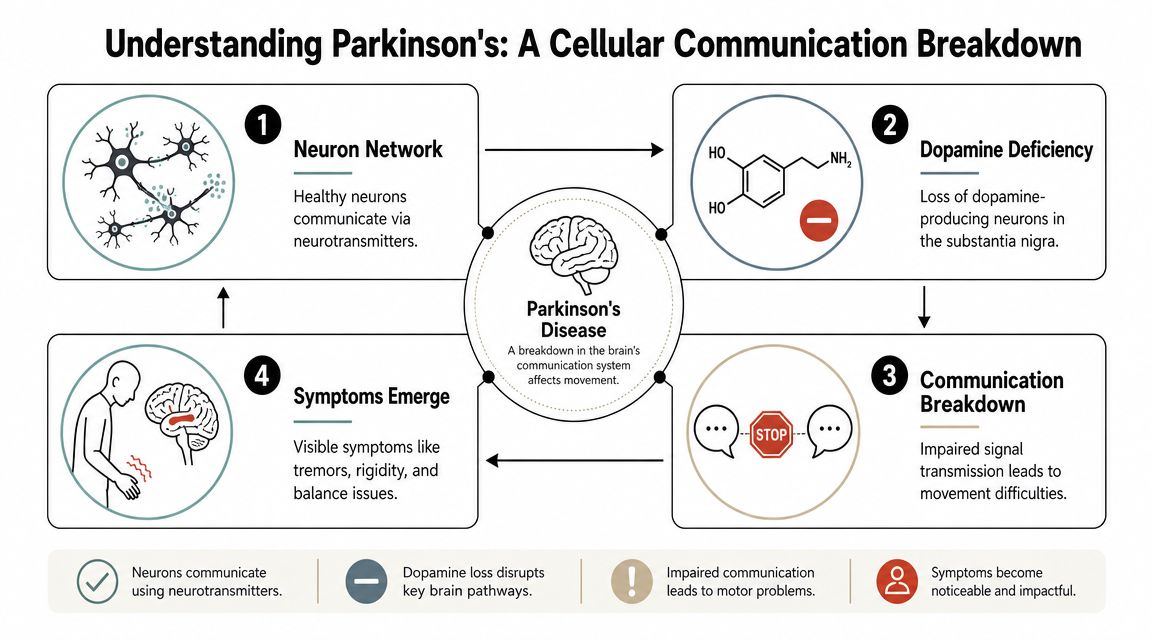
Parkinson's disease is easiest to understand when you stop thinking of it as a vague movement disorder and start thinking of it as a cellular communication problem.
In a healthy brain, networks of nerve cells pass messages with exquisite timing. One of the key messengers is dopamine. Dopamine helps regulate how smoothly the brain starts, sizes, and coordinates movement. When dopamine signaling is strong and well timed, walking, turning, writing, and facial expression happen with much less conscious effort.
In Parkinson's disease, the brain gradually loses dopamine-producing neurons in a region called the substantia nigra. As that supply falls, the motor circuits that depend on dopamine begin to function less efficiently. The result is not paralysis. It's degraded signaling. Movements may become slower, smaller, stiffer, less automatic, and less fluid.
A useful analogy
Think of the dopamine system as a precision delivery service for movement instructions. The brain writes the plan, but dopamine helps deliver that plan to the right destination at the right speed. If the delivery fleet shrinks, messages arrive late, partially, or not at all.
That's why symptoms can look so varied while sharing the same biological core. A hand may tremble at rest. Steps may shorten. Turning may become cautious. Balance may feel less trustworthy. The underlying issue is that the movement network is no longer receiving dopamine support in the way it once did.
For readers who want a broader foundation in regenerative mechanisms, this overview of how stem cell therapy works can help place Parkinson's research in context.
Why standard medications help, but don't fully solve the problem
Most conventional Parkinson's medications are built around one essential idea: increase dopamine signaling or mimic it. That's why many patients experience meaningful symptom relief, especially earlier in the course of disease.
But medication-based dopamine support isn't the same as rebuilding the original cellular architecture. It can help compensate for lost function, yet it doesn't replace the missing dopamine-producing neurons. Over time, patients and clinicians often have to manage timing fluctuations, variable response windows, or symptom patterns that become more complex.
Why stem cells entered the picture
Once you understand that Parkinson's involves the loss of a particular neuron population, the logic of stem cell research becomes clearer. Scientists began asking whether they could generate new dopamine-producing cells and place them where the disease has depleted dopamine supply.
A 2025 review in PubMed Central describes the broader scientific foundation for this effort. In animal models, human pluripotent stem cells, including embryonic stem cells and induced pluripotent stem cells, have been differentiated into dopaminergic neurons and produced substantial motor recovery. The same review also notes that current human trials remain early-stage investigations focused on dose, placement, survival, and side effects, with possible benefits expected mainly in motor symptoms such as tremor, slowness, and stiffness rather than non-motor symptoms.
Parkinson's is not a failure of willpower or effort. It's a disease of impaired signaling inside highly specialized brain circuits.
That single idea explains why movement can feel so frustratingly inconsistent. The intention is there. The cellular messenger system is struggling.
The Two Strategic Goals of Stem Cell Therapy
The phrase stem cell therapy for Parkinson's disease often causes confusion because it refers to two very different therapeutic ambitions. One aims to replace missing dopamine-producing neurons directly. The other aims to support a healthier biological environment around an injured or inflamed nervous system.
Those goals aren't interchangeable. They differ in cell type, delivery method, scientific rationale, and what a patient should realistically expect.

Goal one is direct cell replacement
This is the most technically ambitious strategy in the field. Researchers take stem cells, guide them into becoming midbrain dopaminergic neurons or closely related progenitor cells, and then transplant them into the brain region where dopamine depletion causes motor dysfunction.
The logic is elegant. If Parkinson's disease removes the cells that produce dopamine, perhaps medicine can restore part of that circuitry by implanting new cells designed for that role.
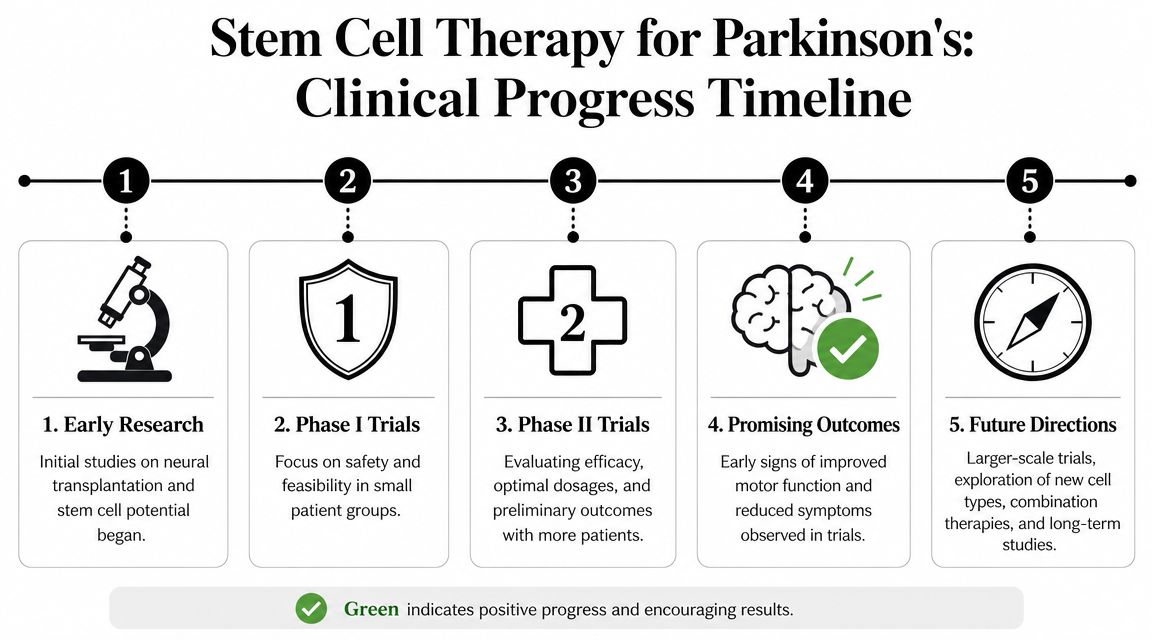
A Mass General Brigham announcement on its Parkinson's stem cell trial explains that stem-cell therapy for Parkinson's disease is being developed primarily as a dopamine-replacement strategy. In the most advanced approaches, cells are reprogrammed into induced pluripotent stem cells and then differentiated into midbrain dopaminergic neurons before transplantation. That phase 1 trial began with its first treated patient on September 9, 2024, and the protocol plans 6 participants with 12+ months of safety and feasibility follow-up.
Later in this section, it helps to see the concept explained visually:
Goal two is systemic support
The second strategy is less about replacing neurons one by one and more about improving the terrain in which neurons live. In regenerative medicine, clinicians often discuss this as creating a more favorable environment for repair, signaling balance, and resilience.
A simple analogy helps. Direct dopamine-cell transplantation is like hiring a highly specialized engineer to fill a very specific role in a failing factory. Systemic support is more like rebuilding the factory's infrastructure: reducing inflammation, improving communication among departments, strengthening maintenance systems, and helping the remaining workforce operate under better conditions.
This broader support model is commonly associated with allogeneic mesenchymal stem cell approaches in regenerative medicine. These cells are not the same as trial-grade dopamine neuron products implanted into the brain. They serve a different purpose and should be understood on their own terms.
For patients exploring broader neurologic applications, this discussion of stem cell therapy for nerve repair offers a useful parallel framework.
Why the distinction matters
Patients often hear the same phrase, “stem cell therapy,” and assume every clinic is pursuing the same science. That's not the case.
Here is the clearest way to separate the two approaches:
| Approach | Primary aim | Typical setting | Main question being tested |
|---|---|---|---|
| Dopamine neuron replacement | Restore missing dopamine-producing cells | Regulated clinical trials | Can transplanted cells survive, integrate, and improve motor function safely? |
| Systemic regenerative support | Improve the biological environment around injured tissue | Broader regenerative medicine settings | Can cell-based signaling support inflammation balance, tissue health, and function? |
Neither should be described as a simple cure. The first is highly specialized and investigational. The second is broader and supportive, not a literal reconstruction of nigrostriatal circuitry.
The most sophisticated patient question isn't “Are stem cells good for Parkinson's?” It's “Which cells, delivered where, for what biological purpose?”
That question protects patients from category errors. It also makes conversations with physicians far more productive.
Current Clinical Evidence and Future Directions
A patient sitting across from me often asks a very fair question: if this science is so promising, what have human trials shown so far?
The honest answer is encouraging, but still early.
What the trials have shown so far
Recent early-stage clinical studies have reported reassuring initial safety findings for stem-cell-derived dopamine neuron transplantation. As noted earlier in the article, investigators have followed participants after implantation and, so far, these reports suggest that the procedure can be carried out without the kind of immediate catastrophic complications that once dominated concern in this field. Some participants have also shown signals of motor improvement, which is why the field has regained serious scientific momentum.
That matters for a simple reason. Before anyone can ask whether transplanted cells improve function in a reliable way, researchers first have to show that the cells can be prepared, implanted, and monitored without dangerous overgrowth or other major transplant-related harm.
A useful analogy is an orchestra returning after a long silence. The first question is not whether the final performance is perfect. The first question is whether the right musicians can get onto the stage, stay in time, and respond to the conductor. In Parkinson's cell therapy, the transplanted dopamine-producing cells are the musicians. Survival, placement, and integration come first. Fine clinical performance comes later.
Why these findings are important, but still preliminary
Phase 1 studies are built to answer narrow, disciplined questions. Can the surgical delivery be performed as intended? Do the implanted cells appear to survive? Are there early warning signs of tumor formation, problematic dyskinesias, immune complications, or other adverse effects? Is there enough signal of benefit to justify larger trials?
Those are important questions, but they are not the same as proving that a therapy works for the broader Parkinson's population over many years.
This distinction protects patients from false certainty. Early positive data can mark the beginning of a real therapeutic path. It does not mean the science is finished, the treatment is established, or the outcome is predictable for every person with Parkinson's disease.
What researchers are trying to solve next
The next phase of progress is less dramatic than a headline, but far more meaningful for patients deciding what deserves their attention.
Researchers are now working through several practical problems that determine whether a cell therapy becomes reproducible medicine rather than an isolated technical success:
Cell dose: how many transplanted cells are needed to produce a meaningful functional effect
Targeting: where those cells should be placed so they have the best chance to connect with existing neural circuits
Manufacturing quality: how to produce cell products that are consistent from one patient batch to the next
Immune management: how to reduce rejection risk while preserving safety
Long-term durability: whether any observed gains persist and whether delayed complications appear years later
Each of these questions is a piece of cellular orchestration. A transplanted neuron is not a standalone fix. It has to arrive in the right place, mature appropriately, communicate with neighboring cells, and behave in a controlled way inside a diseased brain. That is why serious programs move carefully.
For readers who are also considering how regenerative medicine is being studied across other brain-related conditions, our discussion of stem cells for cognitive decline provides a related view of how clinicians think about support, function, and realistic expectations in neurologic care.
At LMI, this is the bridge we want patients to understand clearly. The Parkinson's dopamine-replacement approach being tested in formal trials is investigational and highly specialized. At the same time, the principles guiding responsible regenerative medicine remain consistent across conditions: careful patient selection, respect for biology, attention to safety, and an appreciation that meaningful healing depends on coordination among cells, signals, tissues, and time.
Hope is warranted. Precision is required.
Navigating Treatment Safety and Regulatory Status
Patients often encounter the most confusion at the exact moment they're trying to be proactive. They search for stem cell therapy for Parkinson's disease, see polished websites, and assume that if a treatment is being offered somewhere, it must be established medicine.
It isn't that simple.
What “not FDA approved” actually means
A UCI Health overview of a Parkinson's stem cell clinical trial addresses a major point of confusion: the difference between approved clinical trials and commercial clinic offerings. Key organizations emphasize that there is no FDA-approved stem cell therapy for Parkinson's disease. The same source notes that trial-grade cell products used for dopamine replacement are markedly different from unproven injections at clinics that lack rigorous safety data and do not reliably replace lost neurons.
That statement has direct practical meaning. It means that if someone is advertising a routine stem cell treatment as an established Parkinson's therapy, that claim should trigger careful scrutiny.
Questions every patient should ask
A thoughtful patient doesn't need to become a cell biologist, but they should ask disciplined questions.
What exact cell type is being used? “Stem cells” is too vague.
What is the stated biological goal? Dopamine replacement, inflammatory signaling support, or something else.
Is this part of a regulated clinical trial? If not, what evidence supports the specific protocol?
How are safety, sterility, and quality control documented?
What outcomes are being measured, and over what follow-up period?
If answers remain vague, that's not a minor issue. It's a warning sign.
Red flags to treat seriously
Commercial claims in this area often rely on emotional pressure rather than scientific precision. Be cautious if you hear any of the following:
Guaranteed reversal claims: Parkinson's biology is too complex for certainty-based promises.
One-size-fits-all protocols: Serious neurologic care should be individualized.
No clear distinction between symptom support and neuron replacement: These are different therapeutic categories.
Poor transparency about cell sourcing or laboratory standards: Quality control is not optional.
Marketing language that outruns the evidence: Luxury presentation should never substitute for scientific clarity.
For patients evaluating options abroad, this guide on whether stem cell therapy in Mexico is safe offers a practical framework for assessing standards and oversight.
Safe care begins with intellectual honesty. If a provider can't explain exactly what is being offered and what it is not designed to do, step back.
The Longevity Medical Institute Protocol for Neurological Health
A modern neurologic regenerative program shouldn't be built around a single intervention in isolation. Neurologic function depends on oxygen delivery, inflammatory tone, metabolic health, vascular integrity, sleep, recovery, imaging clarity, and laboratory insight. Cell therapy may be one component of that context, but it is rarely the whole picture.
That principle is especially relevant in chronic neurodegenerative conditions, where the goal is often to improve the body's capacity for resilience and support rather than to claim a direct replacement of specialized brain circuitry outside formal trial settings.
A systems-based approach
Within regenerative medicine, a physician-led neurological protocol may combine several layers of care rather than relying on one headline treatment. In that model, allogeneic stem cell platforms are used as part of a broader cellular support strategy.
Examples of how a thorough program may be structured include:
Allogeneic stem cell selection: Different cell sources may be chosen based on inflammatory, restorative, or signaling goals.
Hyperbaric oxygen therapy: Used to support oxygen delivery and cellular energy dynamics.
Peptide strategies: Applied selectively to support targeted signaling pathways.
Advanced diagnostics: Imaging and laboratory testing help define the patient's baseline and monitor response over time.
Quality matters. Cell-based medicine should be embedded inside a disciplined clinical process, not presented as a standalone luxury add-on.
Why diagnostics shape the plan
Two patients may both carry a Parkinson's diagnosis and still have very different therapeutic priorities. One may struggle most with motor fatigue and exercise tolerance. Another may be limited by sleep disruption, inflammatory burden, or broader metabolic stress.
A complex protocol often depends on tools such as:
| Clinical layer | Why it matters |
|---|---|
| Advanced imaging | Helps clarify structural context and rule in or out competing issues |
| Broad biomarker testing | Reveals inflammatory, metabolic, hormonal, and nutritional patterns |
| Cardiovascular assessment | Supports safe planning in medically complex patients |
| Functional monitoring | Tracks whether the patient is actually moving, sleeping, and recovering better |
That kind of orchestration is one reason many patients look specifically for physician-led stem cell therapy in Mexico rather than commodity-style treatment packages.
What a premium standard of care should feel like
For a patient, premium care shouldn't mean theatrical promises. It should mean careful intake, precise diagnostics, transparent discussion of limitations, and a treatment plan that respects complexity.
A strong neurological regenerative program usually includes:
Clear expectation-setting: Supportive goals are defined transparently.
Layered therapies: Cell therapy, oxygen-based therapies, peptide protocols, and rehabilitation principles are aligned rather than fragmented.
Ongoing reassessment: The plan evolves based on response, not marketing scripts.
In Parkinson's disease, that level of care matters because patients are not simple cases. They are living within a constantly evolving neurological state that requires nuance, patience, and thoughtful medical supervision.
Frequently Asked Questions About Stem Cell Therapy
A common scene plays out in consultation rooms. A patient or family member has read about stem cells, seen headlines about Parkinson's research, and asks a direct question: “Is this real treatment, or is it still experimental?” That question deserves a careful answer, because Parkinson's stem cell science sits at the meeting point of genuine progress and real uncertainty.
Can stem cell therapy cure Parkinson's disease
Stem cell therapy for Parkinson's disease should not be described as a cure at this stage. The most accurate description is an investigational area of medicine. Researchers are testing whether specially prepared cells can help restore lost function, especially through dopamine-cell replacement strategies, but that work is still under formal study.
For patients, this distinction matters. A therapy can be promising and still unproven. In Parkinson's care, honesty about that difference is part of good medicine.
Are the newest clinical trial results encouraging
They are encouraging, and they should be interpreted with discipline. A Keck Medicine overview of emerging Parkinson's stem cell trials describes early findings from studies such as the phase 1 exPDite trial of bemdaneprocel, where the procedure was generally well tolerated, with no serious adverse events linked to the therapy at 18 months. The same report makes the larger point clearly. Researchers are watching for long-term graft survival, safety, and whether transplanted cells integrate well enough to produce meaningful motor benefit.
That is how this field should be understood. Early safety signals are important, but they are not the same as settled clinical success.
If a treatment uses stem cells, does that mean it can replace lost dopamine neurons
No. Stem cells are a broad category, not a single therapy.
The Parkinson's trials receiving the most attention are testing highly specialized, laboratory-directed cells intended to become dopamine-producing neurons after implantation into the brain. That is very different from general regenerative approaches that aim to influence inflammation, signaling, repair support, or the body's recovery environment. The comparison is similar to the difference between replacing a specific musician in an orchestra and improving how the whole orchestra performs together. Both may matter, but they are not the same intervention.
This is one of the most important questions patients can ask, because many commercial claims blur that distinction.
Who should follow this research closely
Patients whose symptoms remain difficult to manage often want to understand what may be coming next. Families also benefit from following the field, especially when they are trying to separate serious clinical development from marketing language. So do patients who are considering supportive regenerative care now and want a realistic view of what is being tested for the future.
A steady, informed attitude helps. Hope is useful. So is patience.
What should I look for in a consultation
Look for a physician who explains the treatment in plain language and can tell you exactly which biological goal is being pursued.
A strong consultation should clarify:
Your current Parkinson's pattern and priorities
Whether the goal is symptom support, functional improvement, or discussion of investigational future options
What type of cells or biologic therapy is being proposed
What published evidence supports that specific approach
What is known, what is unknown, and what alternatives should be considered
If those answers stay vague, the consultation is not precise enough.
Why do some patients still pursue regenerative programs if Parkinson's-specific neuron replacement is still investigational
Because patients live in the present, not only in the future of clinical trials.
Many are seeking better day-to-day function, more physical resilience, steadier recovery, and support for the biological environment in which the nervous system is working. At Longevity Medical Institute, that principle centers on safety, cellular orchestration, and physician-led decision making. The aim is not to present an investigational Parkinson's cure before the science is ready. The aim is to align regenerative strategies with the patient's broader neurological health while respecting the limits of current evidence.
That bridge matters. It connects serious trial science, which is testing whether targeted cells can replace missing neurological function, with the practical reality that patients still need thoughtful care today.
Is it reasonable to feel hopeful and skeptical at the same time
Yes. That is often the healthiest position.
Hope keeps patients engaged with meaningful progress in the field. Skepticism protects them from exaggerated claims, especially in an area where the words “stem cell therapy” can refer to very different treatments with very different goals. In Parkinson's medicine, both are signs of good judgment.
If you're exploring advanced, physician-led regenerative care, Longevity Medical Institute offers personalized programs designed around rigorous diagnostics, allogeneic cellular therapies, and integrated longevity medicine in Los Cabos. Patients seeking a high-touch, medically supervised approach can learn more through the institute's treatments and resources platform at Longevity Medical Institute Treatments & Resources.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: May 22, 2026
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.