What Is a Physiatrist? a Guide to Functional Medicine
A lot of people find a physiatrist only after a frustrating medical loop. Your knee still hurts, your shoulder still catches, your foot pain keeps changing the way you walk, and every visit seems to answer one question while creating two more. One clinician looks at the joint. Another looks at the scan. A therapist focuses on exercise. You're left trying to piece together the full story of why your body doesn't feel or perform the way it should.
That's where a physiatrist can feel different.
This is the specialist many patients wish they'd met earlier. Instead of asking only, “What structure is injured?” a physiatrist also asks, “How is this changing the way you move, compensate, sleep, train, work, and recover?” That shift matters. It turns medicine from a narrow repair job into a functional investigation.
At its best, physiatry sits at the intersection of diagnosis, performance, pain care, and rehabilitation. It's especially valuable for people who want a sophisticated, non-surgical path forward, including active adults, athletes, and patients interested in a more root-cause approach to recovery and longevity.
Your Guide to a New Kind of Medical Specialist
You may be in this position right now. Your back pain started as something minor. Then it spread into the hip. Then your gait changed. Then your workouts became inconsistent, your sleep worsened, and even a long walk started to feel like a negotiation with your body. You saw a few clinicians, got partial answers, and still didn't have a unified plan.
A physiatrist often enters the story at exactly this point.
Think of this doctor as a medical detective for function. They don't just look for damage. They look for the chain reaction. If your foot hurts, they want to know whether your calf mechanics changed, whether your pelvis started compensating, whether a nerve is involved, and whether the underlying problem is less about one painful spot and more about a faulty movement system.
That whole-body perspective is one reason patients value this specialty so highly. It's also one reason access can be difficult. The United States faces a national shortfall of about 940 physiatrists, a 10.6% deficit, according to research on physiatrist workforce shortages. For patients seeking non-surgical care for disability, pain, or impaired mobility, that shortage makes these specialists both important and harder to find.
Why people get confused before they find one
Most patients know what a surgeon does. They usually know what a physical therapist does. A physiatrist sits in a less obvious category, which means many people don't realize this specialty exists until they've already spent months trying to connect the dots themselves.
A good physiatrist doesn't treat your MRI in isolation. They treat the way your body is functioning in real life.
If you've been trying to understand stubborn joint, spine, or nerve symptoms, a practical next step is to review joint and spine pain relief guidance that frames pain through movement, mechanics, and recovery, not just through anatomy.
The Physiatrist as The Body's Functional Architect
A physiatrist is a board-certified medical doctor, either an MD or DO, who completes a four-year residency in Physical Medicine and Rehabilitation, or PM&R. These physicians diagnose conditions and direct non-surgical treatment plans, and they often perform interventional procedures such as ultrasound-guided injections with high precision, as described by this overview of what a physiatrist does.
What functional architect means in real life
An architect doesn't focus on one brick. They study how the full structure works together. A physiatrist does something similar with the body.
They look at the relationship between the brain, nerves, muscles, bones, tendons, and joints. If one part isn't doing its job, another part often overworks to compensate. That's why a person may feel pain in one place while the underlying cause sits somewhere else.
A simple example helps. A patient with shoulder pain may assume the problem is only in the shoulder. A physiatrist may identify a mix of poor scapular control, neck involvement, altered posture, and tendon overload. The treatment plan then becomes more precise because it's built around the entire movement system.
What makes their approach different
Physiatrists are physicians first, which means they can evaluate medical complexity, establish a diagnosis, prescribe treatment, and perform certain procedures. But their goal isn't merely to label a condition. Their core mission is to restore function.
That focus changes the clinical question from “What is wrong?” to “What's limiting your life, and how do we improve it without unnecessary surgery?”
Here's how that usually plays out:
They diagnose strategically. A physiatrist studies pain patterns, weakness, mobility, coordination, and the way symptoms behave during daily activity.
They direct non-surgical care. That may include therapy, medication, bracing, injections, and recovery planning.
They build for independence. The end point isn't just less pain. It's better movement, confidence, resilience, and quality of life.
Practical rule: If your main goal is to move better, hurt less, and avoid surgery if possible, a physiatrist is often the right specialist to evaluate you early.
Common Conditions Addressed by Physiatry
One reason this specialty is so valuable is its range. Physiatry isn't limited to one body part or one stage of recovery. It covers many conditions that interfere with movement, comfort, coordination, and independence.
Spine and joint problems
Many patients first encounter a physiatrist. Common concerns include back pain, neck pain, tendon irritation, joint overload, osteoarthritis, and pain patterns that seem to travel from one area to another.
A physiatrist is useful when pain isn't just pain. Maybe your knee issue changed the way you squat. Maybe your neck symptoms are now causing headaches and arm discomfort. Maybe your foot pain is reducing your stride and aggravating the low back. These are functional patterns, and they respond best when someone looks at the entire chain.
If you're weighing broader options for persistent discomfort, this overview of chronic pain treatment options can help frame where non-surgical rehabilitation fits.
Neurological recovery and spasticity care
Physiatrists also care for patients whose function has changed because of the nervous system. That includes stroke recovery, traumatic brain injury, spinal cord injury, and spasticity that affects comfort and movement quality.
In these cases, the body is a little like an orchestra that has lost its conductor. The muscles may still be present. The limbs may still be capable of movement. But timing, control, and communication have changed. A physiatrist works to improve that coordination and reduce the barriers that keep the body from moving efficiently.
Sports and performance injuries
Active adults often assume they need a sports surgeon for every athletic injury. Sometimes they do. Often they don't.
Physiatrists commonly manage conditions such as rotator cuff tendinopathy, knee osteoarthritis, muscular injuries, and plantar fasciitis through non-operative care. They're especially helpful for people who want to return not just to baseline function, but to training, recreation, and performance with a lower risk of repeated overload.
Why this breadth matters
A physiatrist can be especially helpful when your symptoms don't fit neatly into one box.
Pain plus weakness
Injury plus compensation
Healing tissue plus poor mechanics
A clear scan but ongoing functional limitation
That combination is exactly where PM&R shines. The specialty is designed for patients who need someone to translate anatomy into action.
The Physiatrist's Advanced Diagnostic and Treatment Toolkit
A strong physiatry evaluation goes far beyond “Where does it hurt?” The doctor studies how you stand, walk, recruit muscle, protect painful areas, and lose efficiency under load. In many cases, the body tells the story before the imaging does.
Diagnostic precision matters
A physiatrist often combines a physical examination with targeted diagnostics to answer a more important question than whether something looks abnormal. The question is whether that abnormality explains your symptoms and functional limits.
That's why imaging and testing work best when paired with movement analysis and clinical judgment. In modern integrative care, advanced tools can add another layer of clarity, including AI-enhanced full-body MRI technology for broader structural review and in-house biomarker testing to look at systemic contributors to recovery, inflammation, and resilience.
Ultrasound-guided care and procedural treatment
Physiatrists don't just diagnose. Many perform procedures that help confirm a pain generator, calm irritated tissue, or improve function with greater precision.
According to the AAPM&R description of physiatry procedures, physiatrists administer platelet-rich plasma (PRP), manage spasticity with botulinum toxin injections and intrathecal baclofen pumps, and use ultrasound imaging to guide treatment accurately into joints, muscles, and tendons for conditions such as osteoarthritis and tendinosis.
That precision matters because soft tissue structures sit close together. A guided injection is different from a blind estimate. It's more like placing a key into the exact lock, rather than trying several doors in the hallway.
What treatment planning often includes
A physiatrist's toolkit may include a mix of therapies, depending on the diagnosis and your goals:
Targeted rehabilitation: Specific therapy prescriptions based on the weak link in your movement pattern.
Interventional support: Image-guided injections when a procedure can reduce pain or improve participation in rehab.
Biomechanical correction: Bracing, activity modification, gait changes, and return-to-exercise planning.
Neuromuscular strategy: Spasticity management, coordination work, and nervous-system-focused rehabilitation.
The best treatment plan is specific enough to target the problem, but broad enough to restore the way the whole body works together.
Physiatrist vs Orthopedist vs Physiotherapist
Patients ask this all the time, and the confusion is understandable. These professionals often treat the same body regions, but they don't play the same role.
A useful way to think about it is this. If your body were a high-performance vehicle, the orthopedic surgeon is the structural repair expert, the physical therapist is the movement retraining specialist, and the physiatrist is the physician who studies how the entire system is functioning and directs the best non-surgical path.
Comparing your musculoskeletal care team
The field of physiatry requires at least 12 years of post-high school training, including medical school and a four-year PM&R residency, and it has been recognized as a distinct specialty since 1947, according to this summary of physiatry training and history.
| Attribute | Physiatrist (PM&R Doctor) | Orthopedic Surgeon | Physical Therapist (PT) |
|---|---|---|---|
| Core focus | Function, pain, rehabilitation, non-surgical care | Structural problems that may require surgery | Movement retraining, exercise, mobility |
| Medical degree | Yes, physician | Yes, physician and surgeon | No, not a physician |
| Can diagnose medically | Yes | Yes | Evaluates movement and impairment, but doesn't serve as a physician diagnostician |
| Can prescribe medication | Yes | Yes | No |
| Can order imaging | Yes | Yes | Depends on setting and jurisdiction, but generally not as the treating physician |
| Performs surgery | No | Yes | No |
| Performs injections | Often, especially image-guided procedures | Sometimes, depending on specialty and practice | No |
| Best fit | Complex non-surgical pain or function problems | Fractures, tears, deformity, advanced structural repair needs | Rehab execution, strength, mobility, motor control |
When each one is the right first stop
If you've had a major fracture, obvious instability, or a condition clearly heading toward surgical repair, an orthopedist may be the right first call.
If you already have a diagnosis and need guided exercise, hands-on rehabilitation, and progressive loading, a physical therapist is often essential.
A physiatrist is especially valuable when the case feels less straightforward:
You want to avoid surgery if possible
Pain and function don't match your scan
You have nerve, muscle, and joint symptoms together
You need someone to coordinate rehab with medical treatment
That's also why many patients looking into alternatives to knee replacement surgery benefit from a physiatry perspective before making a final procedural decision.
A physiatrist often acts like the quarterback of non-surgical musculoskeletal care, directing the right play at the right time.
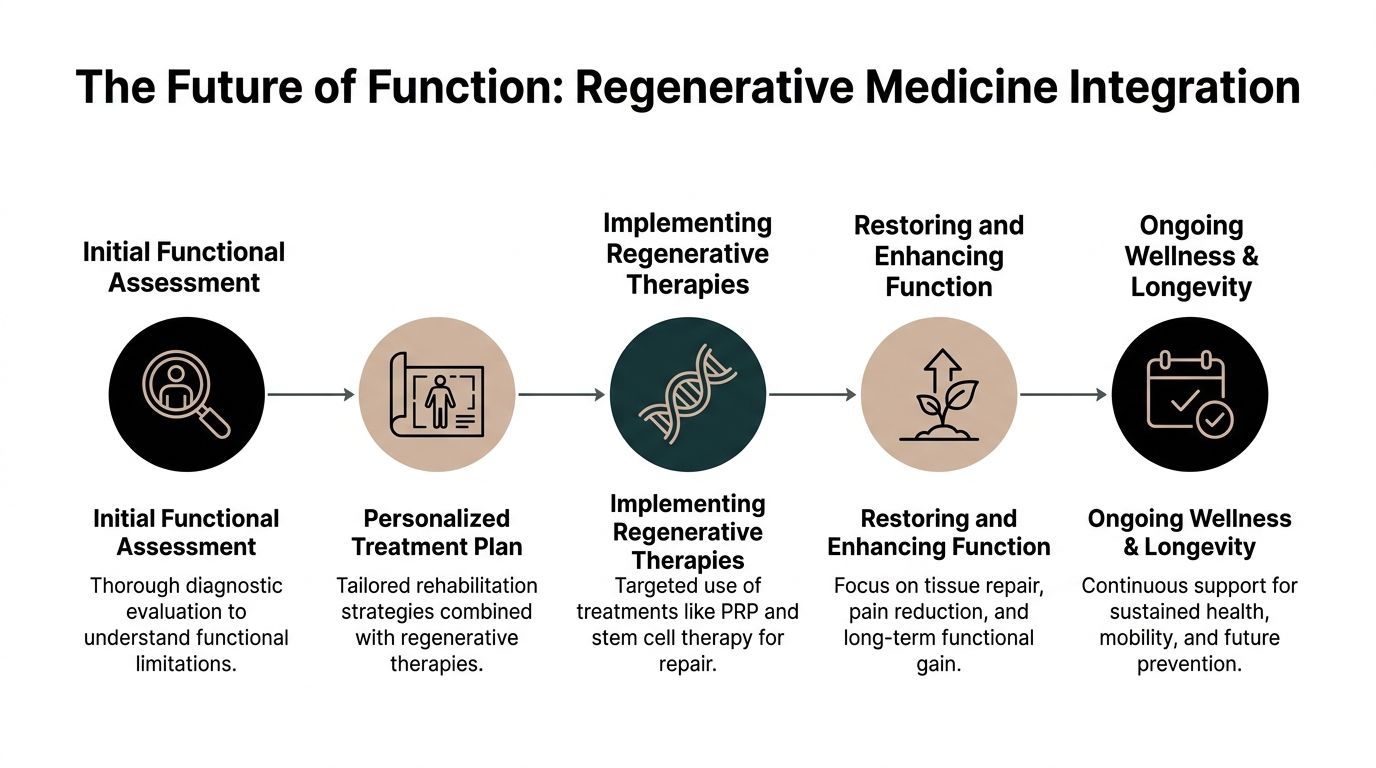
The Future of Function Integrating Regenerative Medicine
Traditional physiatry focuses on restoring movement, reducing pain, and helping people function better without surgery. Regenerative medicine aims at a related but deeper question. Can we also support the biological environment of repair?
That's where many patients get lost. They understand physical therapy. They may have heard of PRP. But once the conversation turns to advanced biologics, stem cells, exosomes, or cellular therapies, the boundaries between specialties become blurry.
A meaningful gap in patient education exists here. As noted in Cleveland Clinic's explanation of physiatrists, people often understand physiatrists in the context of PRP and non-surgical musculoskeletal care, yet the role of a physiatrist in administering or coordinating allogeneic stem cell or exosome protocols for chronic inflammation and orthopedic injuries is often unclear.
Why integration matters
Function and tissue health aren't separate conversations. They're partners.
If rehabilitation is the blueprint for rebuilding a house, regenerative medicine is the work done at the material level. One addresses alignment, stability, and mechanics. The other may support the environment in which healing occurs. Neither is complete on its own when a patient has chronic overload, persistent inflammation, recurrent soft tissue breakdown, or poor recovery capacity.
That integrated view is why more patients are seeking regenerative rehabilitation therapy rather than isolated treatments.
A modern root-cause model
In an advanced setting, a physiatrist can help determine whether a patient needs only movement correction and procedural care, or whether the plan should also include regenerative strategies and broader longevity support.
That may involve:
Precise biologic planning: Physiatrists already work with PRP in musculoskeletal care. In regenerative-focused clinics, that framework may expand into coordinated allogeneic cell-based approaches.
Whole-person recovery: A patient with chronic tendon pain may also have inflammatory load, sleep disruption, impaired conditioning, and poor tissue resilience.
Performance and prevention: The goal isn't only returning to baseline. It's building a body that tolerates life and training better.
For clarity, many regenerative clinics have moved away from discussing autologous stem cells as their primary model and instead focus on allogeneic approaches. In that setting, cell therapy may involve laboratory-produced lines such as placental, Wharton's jelly, adipose, endometrial, and dental pulp stem cells, alongside therapies such as peptides, hyperbaric oxygen, recovery technologies, and blood-based or imaging-based precision diagnostics.
Recovery is stronger when the treatment plan addresses both how you move and how you heal.
Your Path to Recovery What to Expect at Longevity Medical Institute
You should consider a physiatry evaluation when pain keeps returning, when mobility or strength has dropped, when daily life feels smaller because of a musculoskeletal or nerve issue, or when you want a serious non-surgical opinion before moving toward a more invasive intervention.
A thorough first visit should feel organized, not rushed. Expect a detailed history, a functional examination, and a discussion that connects symptoms to real-life limitations. The best evaluations don't stop at naming a diagnosis. They clarify what's driving it, what's prolonging it, and which tools are most appropriate for your next step.
In a premium longevity setting, that may also include broader diagnostics that place joint or nerve symptoms into the context of whole-body health. Depending on the case, that can involve advanced heart evaluation, in-house lab analysis measuring 140 biomarkers, and full-body MRI integration with AI to uncover patterns that a narrower workup might miss.
What a refined patient experience should include
Clarity: You should leave knowing what the problem is likely to be, what still needs confirmation, and what the treatment sequence looks like.
Precision: Image-guided procedures, functional rehabilitation, and regenerative options should be selected for a reason, not offered as a menu.
Continuity: Your care plan should connect pain relief, tissue support, performance restoration, and long-term resilience.
If you've been searching for a specialist who can connect orthopedic pain, neurological function, rehabilitation strategy, and regenerative thinking, a physiatrist may be the missing link.
If you're ready to explore a more complete path to recovery, performance, and healthy aging, Longevity Medical Institute offers physician-led care that blends advanced diagnostics, rehabilitation strategy, and regenerative medicine in one setting.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: July 16, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.