Stem Cell Therapy for Multiple Sclerosis: New Hope
Many people who live with multiple sclerosis know the pattern well. A good week creates hope, then a flare, a new symptom, or a wave of fatigue changes the plan again. You may be doing many things right, working with your neurologist, taking medication, adjusting your schedule, protecting your energy, and still feeling like the deeper problem remains unresolved.
That's often why people start searching for stem cell therapy for multiple sclerosis. Not because they expect a miracle, but because they want a treatment strategy that aims at the biology underneath the symptoms. They want to know whether medicine can do more than react to inflammation after the fact.
Stem cell therapy has changed that conversation. In the MS world, it has opened two very different paths. One is an intensive transplant-based approach designed to reset the immune system. The other is a regenerative approach centered on allogeneic mesenchymal stem cells, with the goal of calming harmful immune activity, supporting nerve tissue, and improving the body's repair environment without high-dose chemotherapy.
That distinction matters. Patients often hear the phrase “stem cell therapy” as if it describes one treatment. It doesn't. In practice, the type of cell, the method of delivery, the treatment goal, and the safety profile can differ substantially. Understanding those differences is the first step toward making a sound decision.
A New Horizon for Multiple Sclerosis
MS rarely feels linear. One person may struggle most with numbness, imbalance, or vision changes. Another may describe a quieter but equally disruptive loss of stamina, concentration, or confidence in daily movement. Even when symptoms are mild on paper, the unpredictability can be exhausting.
Traditional care has made meaningful progress, especially for inflammatory disease activity. But many patients still feel caught between two unsatisfying options. They can manage symptoms and monitor progression, or they can consider more aggressive interventions that may help some people but come with considerable intensity and risk.
Stem cell therapy introduced a new medical idea. Instead of focusing only on suppressing episodes, clinicians began asking whether cellular therapies could change the disease environment itself. Could treatment reduce harmful immune behavior? Could it help protect vulnerable nerve tissue? Could it support repair mechanisms that the body can no longer sustain efficiently on its own?
Stem cell therapy for multiple sclerosis isn't one promise. It's a category of strategies with very different goals.
That's why grounded hope is more useful than hype. The strongest conversations in this field aren't about “curing MS overnight.” They're about identifying which biological pathway a treatment targets, who is most likely to benefit, and what realistic outcomes look like over time.
For some patients, the most important outcome is fewer inflammatory setbacks. For others, it's stability. For others still, it's improved resilience, clearer thinking, better daily function, or a stronger platform for rehabilitation and recovery. A careful regenerative plan should be judged by those real-world goals, not by fantasy language.
Understanding Multiple Sclerosis at the Cellular Level
MS begins with a problem of mistaken identity. Your immune system is designed to protect you. In MS, parts of that system start behaving like a faulty security system that flags your own nervous system as a threat.
The main target is myelin, the protective coating that wraps around nerve fibers. Myelin works like insulation around electrical wiring. When it's intact, signals move efficiently. When it's inflamed or damaged, signals slow down, become distorted, or fail to get through cleanly.
The immune attack
Think of a well-run building with an overreactive alarm team. Instead of stopping intruders, the team starts smashing windows and cutting wires inside the building itself. That's close to what happens in MS. Immune cells trigger inflammation in the brain and spinal cord, and that inflammation damages myelin and sometimes the nerve fibers underneath it.
When that process affects different areas of the central nervous system, symptoms can vary widely. A lesion in one location may affect vision. In another, it may affect balance, bladder function, coordination, sensation, or cognition. This is one reason MS can feel so personal and so inconsistent from one patient to another.
Why symptoms can continue even when inflammation quiets down
Early in the disease, the body may compensate remarkably well. It can reroute signals, reduce symptoms after a relapse, and attempt some repair. Over time, though, repeated inflammatory injury can leave behind more lasting structural stress.
That's where many patients get confused. They hear that MS is “autoimmune,” which is true, but that's only half the story. MS also involves neurodegeneration, meaning the nerve network itself can become less resilient over time. So the illness isn't only about stopping attacks. It's also about protecting tissue that has already been placed under strain.
For a deeper look at this biological balancing act, our guide to immune modulation with stem cells explains why calming the immune response can be central to regenerative care.
Why this matters for treatment decisions
Once you understand those two layers, immune dysfunction and nervous system injury, stem cell therapy makes more sense. A treatment might aim to reset the immune system aggressively. Or it might aim to modulate inflammation, reduce damaging signaling, and support the environment around vulnerable nerve cells.
Clinical perspective: In MS, a treatment can be valuable even if it doesn't "replace" damaged nerves directly. If it reduces inflammatory pressure and improves the repair environment, that can still matter in a meaningful way.
That distinction helps patients ask better questions. Not “Do stem cells fix MS?” but “Which stem cells, for what purpose, and under what clinical circumstances?”
The Two Philosophies of Stem Cell Therapy for MS
Stem cell therapy for multiple sclerosis typically involves two very different treatment philosophies. They share the phrase “stem cell,” but they don't work the same way.
The transplant model
The modern clinical history of stem cell treatment for MS is usually traced to hematopoietic stem cell transplantation, or HSCT. Human studies began appearing in the mid-1990s, and this approach became the best-established stem-cell strategy for highly active disease. The method functions as an immune reset: high-dose chemotherapy ablates the autoreactive immune system, then the patient's own stem cells are reinfused to rebuild it, as described by the VA overview of stem cell therapy for MS.
In a randomized study registered as ClinicalTrials.gov NCT00273364, investigators evaluated autologous unmanipulated peripheral blood stem cell transplantation using cyclophosphamide plus rabbit antithymocyte globulin. The protocol followed patients for 5 years, which reflects how important long-term monitoring has become in this area of MS research.
This transplant strategy is the most established stem-cell approach in MS, especially for carefully selected people with highly active inflammatory disease. But it comes with a serious tradeoff. The conditioning phase is intentionally aggressive, and major clinical organizations note that it carries significant toxicity and life-threatening risks.
The regenerative modulation model
The second philosophy is different in both intention and experience. Instead of destroying the immune system and rebuilding it, this approach uses allogeneic mesenchymal stem cells, often called MSCs, to influence the immune environment more gently while also supporting tissue protection and repair signaling.
You can think of it this way. HSCT is a hard reboot. MSC therapy is more like changing the software conditions inside an unstable system so it operates with less inflammatory chaos.
That doesn't make the two interchangeable. HSCT has the stronger transplant literature in selected patients with active relapsing disease. MSC therapy is generally discussed in regenerative terms: immunomodulation, anti-inflammatory signaling, neuroprotection, and support for tissue recovery.
Comparing the two approaches
| Feature | Autologous HSCT ("Immune Reboot") | Allogeneic MSC Therapy ("Regenerative Modulation") |
|---|---|---|
| Core goal | Reset the immune system | Calm harmful immune signaling and support repair conditions |
| Cell source | Patient's own blood-forming stem cells | Donor-derived mesenchymal stem cells |
| Conditioning | Requires high-dose chemotherapy | Does not rely on high-dose chemotherapy |
| Clinical experience | Best-established stem-cell approach for highly active MS | Regenerative approach used to support modulation and recovery |
| Primary treatment logic | Eliminate autoreactive immune repertoire, then rebuild | Influence inflammation, trophic signaling, and tissue environment |
| Risk profile | Significant toxicity and serious risks from conditioning | Different safety profile, focused on non-ablative care |
| Typical patient question | “Do I need an immune reset?” | “Can I support stability and repair without ablation?” |
Patients often assume all stem cell therapies for MS are versions of the same procedure. They aren't.
For people considering a non-ablative path, the appeal is clear. They may want a strategy that targets inflammation and tissue stress without entering a chemotherapy-based transplant process. That's where allogeneic MSC protocols have drawn growing attention.
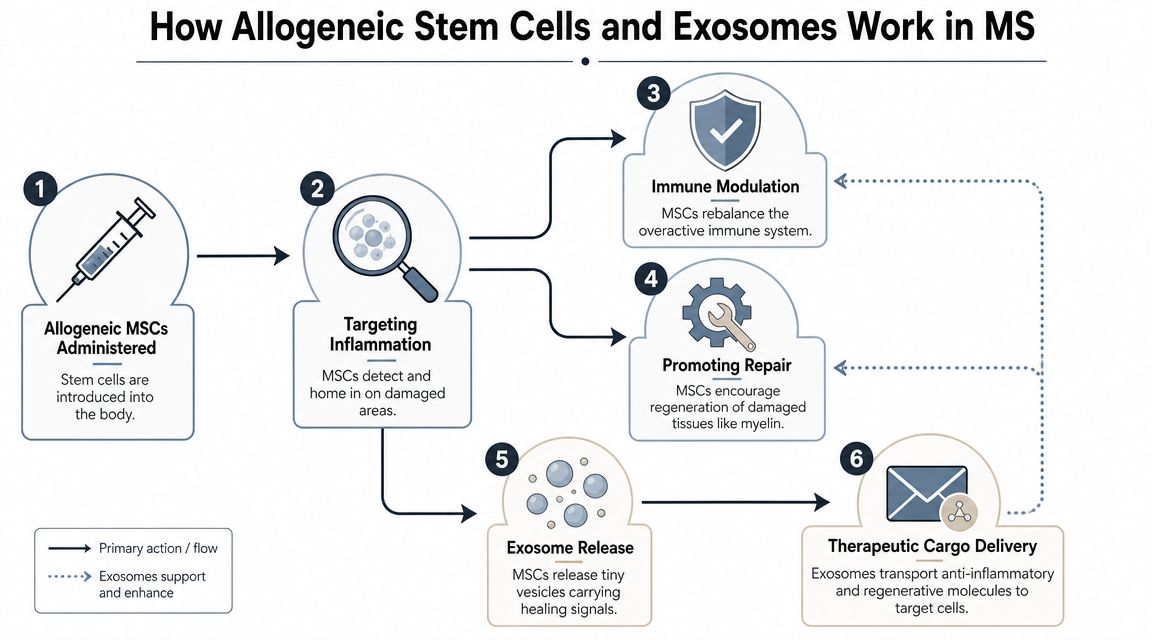
How Allogeneic Stem Cells and Exosomes Work
A person with MS may hear the phrase “stem cell therapy” and picture replacement. New cells go in, damaged cells get swapped out, and function returns. That image is understandable, but it does not reflect how allogeneic mesenchymal stem cells, or MSCs, are believed to help in most regenerative MS protocols.
Allogeneic MSCs work more like expert conductors in a strained orchestra. They do not merely replace injured tissue. They influence the signals around immune cells, nerve cells, and support cells so the system can shift away from chronic inflammatory disruption and toward a more repair-friendly state.
What MSCs are doing
MS is driven by a harmful interaction between immune activity and the central nervous system. The therapeutic aim with MSCs is to soften that interaction. Research has focused on their ability to influence inflammation, release supportive growth factors, and improve the biologic conditions that surround stressed neural tissue, as discussed in the review of stem cell mechanisms and recent MS findings.
This point often clears up a common misunderstanding. MSC therapy is not best understood as a direct myelin replacement procedure. Its value may come from changing the cellular environment so that inflammation is less destructive, vulnerable cells receive more support, and the body has a better opportunity to maintain function and support repair.
That distinction matters because it separates regenerative MSC care from the better-known aHSCT model. aHSCT is designed around immune ablation and rebuilding. Allogeneic MSC treatment is designed around immunomodulation, neuroprotection, and support for the body's own repair capacity, without relying on high-dose chemotherapy.
At Longevity Medical Institute, MS protocols are built around allogeneic cell products rather than autologous harvesting. The in-house biotechnology lab produces five stem cell types: placental, Wharton's jelly, adipose, endometrial, and dental pulp. For clinicians, that wider toolkit creates room to choose cell sources based on the patient's inflammatory patterns, neurologic burden, and treatment goals instead of treating every case as biologically identical.
Why exosomes matter
Exosomes are a major part of why MSC therapy attracts so much clinical interest. If MSCs are the conductors, exosomes are the signals that carry the score to the rest of the orchestra. These microscopic vesicles contain proteins, lipids, and genetic signaling material that can influence how nearby cells behave.
In practical terms, that means the benefit of treatment may depend less on long-term cell replacement and more on communication. Exosomes help explain how MSC-based care may calm inflammatory signaling, support immune balance, and promote a more protective environment for nervous tissue.
Patients often ask whether exosomes and stem cells are competing options or complementary tools. Our guide to the difference between exosomes and stem cells in regenerative treatment explains how they differ and why they are often considered together.
A short visual overview helps make that easier to picture.
What recent research suggests
The most accurate summary is careful and measured. In MS, stem cell based treatment may support immune calming, nerve-supportive signaling, and some degree of regenerative influence. Early and emerging studies have reported encouraging safety findings and signals that point toward neuroprotection in some settings, but that is different from proving that lost neurologic function can be fully restored.
For many patients, this is still meaningful. Slower progression, better biologic stability, reduced inflammatory stress, and support for tissue resilience can matter even when treatment is not a cure.
Why cell diversity can matter in personalized care
Different MSC sources may offer different practical strengths for clinicians designing an individualized program. One patient may need a stronger focus on systemic inflammatory control. Another may need a plan shaped more around neurotrophic support, recovery conditions, or adjunctive regenerative therapies.
A personalized protocol often considers:
Disease pattern: Relapsing inflammatory disease and more advanced progressive disease create different treatment priorities.
Current burden: Fatigue, mobility changes, cognitive symptoms, and baseline function help define what success should look like.
Supportive strategy: Exosomes, peptides, hyperbaric oxygen, and rehabilitation planning may be layered around cell therapy as part of one coordinated regenerative plan.
The strongest regenerative programs do not expect one product to solve every problem. They build biologic support from several angles.
Your Personalized Treatment Program at LMI
A thoughtful MS program begins long before any infusion. The first priority is deciding whether treatment makes sense for the specific person in front of you. Candidacy matters because stem cell therapy tends to perform differently depending on disease stage, inflammatory activity, disability level, and clinical history.
The clearest evidence for stem-cell benefit in MS has been seen in people with highly active relapsing disease, particularly those who haven't responded to or can't take high-efficacy disease-modifying therapy, are under 50, have had MS for 10 years or less, and have low-to-moderate disability, as outlined by the MS International Federation guidance on stem cell therapy for MS. Even outside transplant-based care, that principle still applies. The better the evaluation, the better the treatment logic.
The evaluation phase
A premium medical program shouldn't guess. It should build a baseline.
That usually means reviewing prior MRI findings, relapse history, medication exposure, gait or mobility concerns, fatigue patterns, cognitive complaints, and inflammatory clues from laboratory work. At LMI, this process can be expanded with an in-house clinical lab measuring 120 biomarkers, plus AI-integrated full-body MRI and advanced cardiovascular assessment. Those tools don't diagnose MS in isolation, but they can help define the broader physiologic terrain in which recovery and resilience either struggle or improve.
For patients traveling from the U.S. or Canada, this level of preparation is often one of the biggest differences between a generic infusion center and a physician-led regenerative program. Our overview of physician-led stem cell therapy in Mexico explains why that distinction matters.
Building the treatment plan
One patient may need a protocol aimed mainly at immune balance and inflammatory control. Another may need a broader strategy that supports neurologic resilience, mitochondrial function, oxygen delivery, sleep quality, and physical recovery capacity.
That's why a personalized program often combines multiple layers of care rather than relying on a single event.
A typical treatment design may include:
Allogeneic MSC selection: The physician chooses among placental, Wharton's jelly, adipose, endometrial, and dental pulp cell lines based on the patient's profile and treatment goals.
Exosome support: Exosomes may be used to amplify signaling effects around inflammation control and tissue support.
Adjunctive therapies: Peptides, IV therapies, and hyperbaric oxygen can be added to improve the biologic environment in which regenerative signaling occurs.
Monitoring strategy: Functional changes, symptom trends, energy, cognition, and imaging are tracked over time rather than judged in a single week.
What the treatment experience often looks like
Many patients expect something dramatic. In reality, a regenerative MS protocol is usually more measured. The treatment itself may feel straightforward compared with the complexity of the science behind it.
What matters more is the orchestration around it. Timing, route of administration, supportive therapies, follow-up structure, and post-treatment recommendations all shape the final outcome. Some patients are looking for stability and fewer setbacks. Others hope for better stamina, steadier walking, improved recovery after exertion, or sharper day-to-day function.
Practical rule: The right question isn't "How many cells do I need?" It's "What biologic problem are we trying to solve, and how will we measure progress?"
After treatment
Post-treatment care is where many weaker programs fall short. MS is not a condition that should be approached with a one-day mindset.
A stronger model includes follow-up conversations, symptom tracking, repeat diagnostics when appropriate, and integration with the patient's existing neurology care. Lifestyle factors also matter. Sleep disruption, chronic stress, deconditioning, poor metabolic health, and untreated inflammation elsewhere in the body can all work against a regenerative plan.
Patients often do best when they understand that treatment is part of a larger clinical arc. The infusion may start the process. Recovery habits, monitoring, and supportive care help sustain it.
Safety, Regulation, and Realistic Outcomes
The most responsible discussion of stem cell therapy for multiple sclerosis starts with restraint. This is not a proven cure for MS. It is a developing therapeutic category with some encouraging safety signals, strong biologic rationale, and meaningful differences between treatment models.
What safety data tells us
A notable safety milestone came from a first-in-human phase I study of human neural stem cells in secondary progressive MS. The trial enrolled 15 participants, tested dose levels of 5 million, 10 million, 16 million, and 24 million cells, and followed patients for 12 months. The treatment was reported as safe and well tolerated, with no treatment-related deaths or major adverse events, and no relapses during follow-up, according to MS Canada's summary of the progressive MS neural stem cell study.
That doesn't prove all stem-cell approaches are equally safe. It does show that carefully designed human studies in progressive MS can produce concrete safety data rather than speculation.
What realistic outcomes look like
Patients deserve clear language here. The most reasonable goals in regenerative MS care may include:
Disease stability: Holding the line can be a meaningful clinical win, especially in progressive patterns.
Reduced inflammatory burden: Some therapies aim to calm the immune environment rather than reverse established damage.
Improved function: Energy, recovery tolerance, cognition, or daily physical capacity may improve for some patients.
Better quality of life: Even modest gains can matter if they improve work, movement, confidence, or independence.
What shouldn't be promised is guaranteed reversal of disability. Current research still leaves open major questions about durability, ideal timing, ideal cell type, and which patients benefit most.
Patients should be wary of any clinic that talks about certainty in a field that still requires careful follow-up and honest outcome tracking.
Regulation and why process matters
The regulatory conversation can be confusing for medical travelers. Patients often assume “available” means “unregulated,” or that “regulated” means identical standards everywhere. Neither assumption is reliable.
What matters in practice is whether the clinic operates within a legitimate medical framework, uses rigorous quality controls, maintains clear physician oversight, and communicates transparently about what is known and what is still investigational. If you're evaluating treatment abroad, our guide on whether stem cell therapy in Mexico is safe outlines the questions worth asking before you commit.
A strong program will discuss product sourcing, clinical monitoring, treatment rationale, informed consent, and post-treatment follow-up with the same seriousness it gives to the procedure itself.
Reclaim Your Vitality with Regenerative Medicine
MS changes enough of daily life that patients often stop asking for perfection and start asking for possibility. That's a wise shift. The most meaningful promise of regenerative medicine is not fantasy. It's the chance to approach MS more proactively by targeting immune imbalance, inflammatory signaling, and neurologic support at the same time.
Allogeneic stem cell therapy offers a modern path for people who want to explore care beyond symptom management alone, especially if they're looking for a non-ablative strategy rather than a chemotherapy-based immune reset. In the right setting, with careful selection and structured follow-up, this approach can become part of a broader plan to support stability, function, and resilience.
Patients interested in whole-person recovery often also explore therapies tied to long-term performance and healthy aging. Our article on stem cell therapy for anti-aging and longevity offers additional context on how regenerative care fits into a larger healthspan strategy.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: May 19, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.
Frequently Asked Questions
How do I know if I'm a candidate for stem cell therapy for multiple sclerosis
Candidacy starts with disease pattern, not optimism alone. A physician should review whether your MS is predominantly relapsing and inflammatory or more advanced and progressive, along with your MRI history, symptom course, disability level, prior treatments, and overall health. That evaluation helps determine whether a regenerative approach has a reasonable rationale in your case.
Is this the same as a bone marrow transplant for MS
No. Patients often group all stem cell therapies together, but they aren't the same. The transplant-based immune reset approach uses a very different process and risk profile. Allogeneic MSC therapy is generally discussed as a non-ablative regenerative strategy aimed at immunomodulation, tissue support, and neuroprotection rather than chemotherapy-based immune destruction.
What kind of results should I realistically expect
The best approach is to think in terms of goals, not guarantees. Depending on the patient, those goals may include greater stability, fewer inflammatory setbacks, better energy, improved recovery capacity, or stronger day-to-day function.
Long-term expectations also need to stay grounded. Improvements in disability seen in some stem cell trials don't last for everyone, and worsening can occur in later years. That's why durability remains an important research question and why follow-up matters so much after treatment.
How long should monitoring continue after treatment
Longer than many patients expect. MS is dynamic, and response to treatment may unfold gradually. A credible program should include ongoing communication, symptom tracking, and coordination with your neurology team when appropriate. Monitoring helps distinguish a short-term fluctuation from a meaningful clinical change.
Can I travel from the U.S. or Canada for treatment
Yes, many patients do. The important part goes beyond getting to the clinic. It's making sure the medical review happens in advance, records are assessed carefully, travel is planned around your physical needs, and follow-up is organized before you leave home. Medical travel works best when logistics and clinical decision-making are integrated.
Will I need other therapies along with stem cells
Often, yes. Regenerative medicine usually works best as part of a broader plan. Depending on your needs, that may include exosomes, peptides, hyperbaric oxygen, sleep optimization, nutrition support, rehabilitation, and detailed biomarker tracking. The goal is to improve the biologic environment, not just administer one product and hope for the best.
Is one treatment enough
Sometimes a patient may respond well to a single treatment cycle. In other cases, physicians may consider staged care and longer observation. There isn't a universal formula. The right timeline depends on your baseline condition, treatment goals, and how your body responds over time.
If you're exploring whether regenerative care may fit your MS journey, Longevity Medical Institute offers physician-guided consultations designed to review your history, imaging, and goals with clarity. The right next step is a careful candidacy discussion, not a rushed promise.