Advanced Stem Cell Therapy for Shoulder Injuries
Shoulder pain changes the rhythm of an ordinary day. You feel it when you reach for a seatbelt, lift a carry-on, pull on a shirt, or try to sleep without waking when you roll onto the wrong side. For active adults, it also creates a more private frustration. You may still look healthy, but your world subtly narrows.
Many individuals arrive at this point after doing what they were told to do. They rested. They tried physical therapy. They may have had a cortisone shot that calmed things down for a while, only for the pain to return when they resumed golf, tennis, weight training, swimming, or overhead work. The usual cycle is symptom relief, then reinjury, then a more serious conversation about surgery.
Regenerative medicine offers a different objective. Instead of asking how to mute the shoulder long enough to get through the next few months, it asks whether the damaged tissue environment can be improved so the joint has a real chance to recover. That distinction matters. A shoulder with chronic inflammation, tendon degeneration, or an early tear rarely needs more masking. It needs a better repair signal.
Reimagining Your Recovery from Shoulder Pain
A common scenario is the patient who says, “It’s not one big injury. It’s years of wear, and now everything hurts.” That’s often true. Shoulder problems usually build in layers. A small rotator cuff strain leads to altered mechanics. Then bursitis develops. Sleep gets worse. Training changes. The neck and upper back start compensating. Soon the shoulder feels unreliable, not just painful.
What makes this difficult is that standard care often separates pain from tissue quality. If pain decreases for a few weeks, treatment may be labeled a success even when the tendon, capsule, or joint lining remains biologically irritated. Patients feel that disconnect quickly. They know the shoulder still catches, aches, or fatigues under load.
Why symptom management often falls short
Cortisone can reduce inflammation, but it doesn't rebuild a degenerative tendon. Rest may calm an aggravated shoulder, but it doesn't necessarily improve the tendon-to-bone interface that has been under strain for years. Physical therapy is valuable, especially when mechanics are poor, but therapy works best when the tissue can respond to the load being applied.
Practical rule: If a shoulder improves only while activity is reduced, but flares as soon as normal use resumes, the issue usually isn't just pain sensitivity. The tissue itself may need better biologic support.
In this context, stem cell therapy for shoulder injuries becomes relevant. The aim isn't to “numb and resume.” The aim is to create a local environment that supports repair, reduces inflammatory signaling, and helps the shoulder tolerate movement again.
A more useful goal
The right question isn't whether regenerative medicine replaces every other treatment. It doesn't. The right question is whether your shoulder problem is one of the many conditions where a biologic approach makes more sense before escalating to surgery.
For the right patient, that can mean moving from a management mindset to a rebuilding mindset. Not overnight, and not by magic, but by giving the shoulder a more favorable healing context than it has now.
The Science of Allogeneic Stem Cells and Exosomes
People hear “stem cells” and often imagine one mysterious substance that does everything. In practice, the science is more precise than that. Think of stem cells as master repair coordinators. They don’t arrive to then turn into a brand-new shoulder. Their main value is that they release signals that influence inflammation, cellular communication, and tissue remodeling.
Exosomes are part of that signaling system. If stem cells are the architects, exosomes are the packets of instructions they send to nearby cells. Those messages can influence how the local tissue responds to injury, irritation, and repair.
Patients who want a deeper distinction between these two tools can review this explanation of exosomes vs stem cells.
Why allogeneic cells matter
At our clinic, the discussion starts with one important choice. We use allogeneic cells, not autologous cells. That means the cells come from carefully screened donor-derived tissues rather than being harvested from the patient during the visit.
That matters for a few reasons:
No harvest procedure for the patient means no additional liposuction or bone marrow aspiration.
Younger, highly active cell sources can offer a more consistent biologic product than cells taken from a patient whose own tissues may already reflect age, inflammation, or orthopedic wear.
Lab control matters because cell handling, screening, and preparation directly affect consistency.
Our biotechnology lab produces five different stem cell types: placental, Wharton's jelly, adipose, endometrial, and dental pulp. Those sources aren't interchangeable buzzwords. Each offers distinct biologic characteristics, and the treatment plan depends on the tissue target, the degree of degeneration, and the broader inflammatory picture.
What these cells are doing in the shoulder
In practical terms, allogeneic mesenchymal signaling cells are used because they can help calm swelling, influence the local immune response, and stimulate endogenous repair. In shoulder care, that matters most at the places where healing often stalls: irritated tendons, partial tears, inflamed bursae, and worn joint surfaces.
They also support a treatment philosophy that is more precise than “inject and hope.” The shoulder is a compact joint with several common pain generators packed close together. The supraspinatus tendon, subacromial bursa, glenohumeral joint, biceps tendon sheath, and labrum can all contribute. Biologic therapy works best when the diagnosis is exact and the delivery is exact.
A short visual overview helps make that biology easier to understand:
What patients often misunderstand
The common misconception is that stem cells are only useful if they physically become a new tendon or cartilage surface. That’s too narrow. Much of the clinical effect appears to come from signaling, not simple tissue replacement. The treatment can shift the local environment from irritated and stagnant toward one that is more capable of organized healing.
The shoulder doesn't need random growth. It needs the right biologic message in the right place, delivered with precision.
This is also why source quality and processing standards matter. If you're evaluating stem cell therapy for shoulder injuries, ask where the cells come from, how they're screened, how they're prepared, and how the physician decides which tissue planes to target. Those details separate a real orthopedic biologic protocol from a generic wellness add-on.
Which Shoulder Injuries Respond Best to Stem Cells
A shoulder can hurt for the same reason a luxury car can ride poorly. The symptom is obvious. The failing part is not. In regenerative medicine, outcomes improve when the biologic matches the tissue problem, the injection is placed with precision, and the rehabilitation plan fits the mechanics of that injury.
At Longevity Medical Institute, that selection process is stricter than what many patients encounter in medical tourism settings. We use high-potency allogeneic cell products, AI-integrated imaging review, and a multidisciplinary workup to decide whether a shoulder is a good biologic candidate, a poor candidate, or a case that needs surgery first. That distinction protects patients from receiving an elegant treatment for the wrong diagnosis.
Rotator cuff tears
Rotator cuff pathology is often the strongest indication, especially with partial-thickness tearing and chronic degenerative change. These tendons live in a relatively low-blood-supply environment near their insertion on bone, so they often linger in an irritated, under-repaired state.
That matters because a partial tear still has structural continuity. The tissue is damaged, but not absent. In that setting, a regenerative protocol aims to calm destructive signaling and improve the conditions for organized tendon remodeling while the patient follows a measured loading program.
Large full-thickness tears are different. Some patients still benefit from biologic support for pain or surrounding tissue quality, but a retracted tendon with major loss of mechanics is not the same problem as a smaller contained tear. For patients comparing options in detail, our guide to stem cell therapy for rotator cuff tear explains where biologics fit and where they do not.
Chronic tendonitis and tendinopathy
Many patients are told they have inflammation when the larger issue is failed tendon remodeling. The fibers are disorganized. Load tolerance is poor. The tendon becomes reactive with overhead use, sleep position, or gym activity, then settles just enough to create a false sense of progress.
These cases can respond well when the diagnosis is specific. Supraspinatus tendinopathy behaves differently from biceps sheath irritation, and both differ from pain driven by the subacromial bursa. A premium protocol should separate those structures rather than treating the whole shoulder as one undifferentiated sore area.
I tell patients to picture worn rope fibers, not a simple swollen muscle. The treatment goal is to improve the local repair environment and pair it with intelligent rehab, not just mute pain for a few weeks.
Shoulder osteoarthritis
Shoulder arthritis can also respond, but the goal has to be realistic. Biologics do not turn an arthritic joint into a pristine one. They may improve synovial irritation, reduce pain, and support better day-to-day function in the right patient.
The best candidates usually have earlier-stage degeneration, preserved joint mechanics, and symptoms that still track to inflammation and capsular irritation rather than severe collapse. In advanced arthritis with major bone-on-bone wear, motion loss, and night pain that dominates daily life, surgery remains part of the conversation.
Labral pathology and mixed shoulder pain
Labral findings deserve caution. In adults, a labral abnormality on MRI is often only part of the story. The shoulder may also have cuff overload, biceps irritation, bursitis, or early joint wear.
If the labrum looks abnormal on imaging but the primary pain driver is the cuff and bursa, treating the MRI finding instead of the shoulder exam leads to poor decisions.
LMI’s diagnostic model offers significant value. AI-assisted imaging review helps organize the picture, but it does not replace the physical exam, movement testing, or ultrasound-guided correlation of symptoms to tissue. The point is to identify the true source of pain, not merely what appears on a report.
Who tends to be a stronger candidate
Patients who do best usually have several features in common:
A clear tissue target, such as a partial cuff tear, focal tendinopathy, or early arthritic change
Symptoms that match the imaging and exam, rather than vague whole-arm pain with no consistent source
Failure of appropriate conservative care, including physical therapy, activity modification, or short-lived relief from standard injections
Enough remaining structure to repair, rather than massive retracted tearing or severe mechanical instability
Commitment to rehabilitation, because biologic treatment supports healing but does not replace it
Some shoulders should not be pushed into a stem cell protocol. Severe instability, major mechanical collapse, and large retracted tears often need a surgical plan or at least a surgical opinion. Good regenerative medicine includes saying no when the indication is wrong.
Your Regenerative Treatment Protocol at LMI
The quality of a shoulder injection depends on the quality of the work done before the needle ever touches the skin. A careful protocol starts by deciding whether the shoulder is the primary problem, whether the pathology is focal or diffuse, and whether the patient’s systemic health is helping or interfering with recovery.
Step one is diagnostic clarity
A premium regenerative protocol isn't just an injection appointment. It begins with history, physical examination, musculoskeletal ultrasound, and when needed, advanced imaging to define the problem with precision. At LMI, that can also include an in-house clinical lab measuring over 120 biomarkers and AI-integrated MRI imaging review to identify broader drivers of poor healing such as inflammatory load, metabolic stress, or overlooked adjacent pathology.
That matters because a shoulder that won't heal isn't always failing for local reasons alone. Some patients have impaired recovery because sleep, inflammation, training load, hormonal changes, or systemic stress are distorting the repair environment.
Step two is selecting the right biologic strategy
Once the target is clear, the physician chooses the most appropriate allogeneic cell approach and whether exosomes or other supportive modalities belong in the plan. The decision isn't based on trend language. It’s based on tissue type, severity, chronicity, and whether the problem is more tendon-dominant, joint-dominant, or mixed.
In practical terms, the procedure involves a precise ultrasound-guided injection of allogeneic mesenchymal stem cells into the injured area, and this minimally invasive outpatient approach leads to roughly 80% to 85% of patients achieving marked pain relief and functional improvement within 2 to 4 months.
For patients comparing clinic models and physician involvement, this overview of physician-led stem cell therapy in Mexico explains what to look for in procedural oversight and safety standards.
What the procedure feels like
The actual treatment is usually straightforward. The shoulder is examined again in real time with ultrasound. The physician identifies the exact tissue plane being treated, whether that is the tendon, the joint, or another involved structure. The injection is then performed with imaging guidance rather than anatomical guesswork.
Most patients tolerate this well because it is not an open surgical event. It is a focused outpatient procedure built around precision.
The difference between “a shoulder injection” and a real orthopedic biologic procedure is accuracy. The target matters as much as the product.
Why multidisciplinary care can improve the result
A shoulder rarely fails in isolation. Recovery is often stronger when the injection is integrated into a larger plan that addresses movement, inflammation, training modification, and tissue support. Depending on the patient, that may include physical medicine, peptide strategies, hyperbaric oxygen, or a broader longevity workup.
That doesn't mean every patient needs every tool. It means the protocol should reflect the person in front of you, not a standard menu.
Recovery Timelines and Long-Term Expectations
One advantage of regenerative treatment is that recovery usually looks very different from surgical recovery. That doesn't mean results are instant. It means the process is less disruptive and more biologically progressive.
The first days and first weeks
Right after treatment, many patients can use the arm for light daily activity. The shoulder may feel sore or full for a short period, especially if an already irritated tendon or joint has been treated. That early phase is not the final result. It is the opening phase of a remodeling process.
In the first few weeks, the main job is to protect the treatment zone from the kind of overload that created the problem in the first place. That often means strategic modification, not complete inactivity.
When improvement usually becomes clearer
The next phase is where people often start to notice meaningful changes in pain, sleep, and confidence with movement. The shoulder may feel less reactive with ordinary tasks before it feels fully reliable under higher demand. That sequence is normal.
Patients frequently ask whether they should judge the treatment early. Usually, the better answer is no. Biologic care rarely follows the timeline of a numbing injection. It tends to build.
A useful reference point is this overview of recovery time after stem cell injection, which explains why shoulder improvement is often measured in stages rather than in days.
What to expect long term
Long-term durability is the right question to ask, and the honest answer is nuanced. Numerous animal studies and short-term human trials show promising reductions in inflammation and improved tissue formation, but extensive human clinical data on 2 to 5 year success rates are still emerging. Most patients experience optimal benefits within several months, and the process should be viewed as a progressive healing journey.
That is exactly how I frame it clinically. The treatment has real promise. It also deserves realistic expectations.
A balanced way to think about results
Best-case scenario is reduced pain, stronger function, better tolerance for activity, and delayed or avoided surgery.
Middle ground is partial improvement that still changes daily life in a meaningful way.
Less favorable cases include shoulders with advanced structural failure, poor rehab compliance, or pain sources that weren't fully identified before treatment.
A regenerative procedure should be judged by function over time, not by whether the shoulder feels dramatically different in the first few days.
Stem Cells vs Surgery and Other Shoulder Treatments
A patient sits across from me after months of shoulder pain, holding an MRI report in one hand and a surgical consult in the other. The question is rarely, “Do stem cells work?” The question is whether a biologic procedure is the right choice compared with cortisone, PRP, physical therapy, or an operation.
The answer depends on what is driving the pain. A tendon with chronic degeneration is different from a frozen shoulder. A labral injury in an overhead athlete is different from advanced arthritis. At Longevity Medical Institute, we do not treat those as the same problem merely because they all hurt in the same region. Our process uses AI-supported diagnostic review, image-guided assessment, and coordinated input from regenerative medicine, rehabilitation, and functional care so the treatment choice matches the biology and mechanics of the joint.
Cortisone
Cortisone can calm an inflamed shoulder quickly. That can help someone sleep, travel, or tolerate early rehabilitation.
Its limitation is straightforward. It suppresses inflammation, but it does not improve tendon quality, restore cartilage, or correct the mechanical pattern that keeps irritating the joint. For a patient who wants durable tissue improvement, cortisone is usually a temporary tool, not a long-range strategy.
PRP
PRP can be useful in the right case. It concentrates platelet-derived signaling proteins and may help with milder tendon injuries, early irritation, or as an adjunct to a broader plan.
But PRP has a ceiling. If the shoulder has more advanced degeneration, recurrent inflammation, or a poor healing environment, platelets alone may not provide enough biologic direction. That is where our use of high-potency allogeneic stem cells and exosome support can offer a wider regenerative signal than standard injection options often available to medical tourists.
Surgery
Surgery still has a clear role. Large full-thickness tears, significant instability, fracture-related problems, and severe structural failure may need operative repair.
What I tell patients is simpler than the usual sales pitch on either side. Surgery can be appropriate, but it comes with anesthesia, immobilization, scar formation, a longer rehabilitation arc, and the possibility that pain or weakness will not fully resolve even after technically successful repair. Regenerative treatment is not a replacement for every operation. It is an attempt to improve the tissue environment before cutting, or to avoid cutting when the shoulder still has a realistic capacity to recover.
Side-by-side decision view
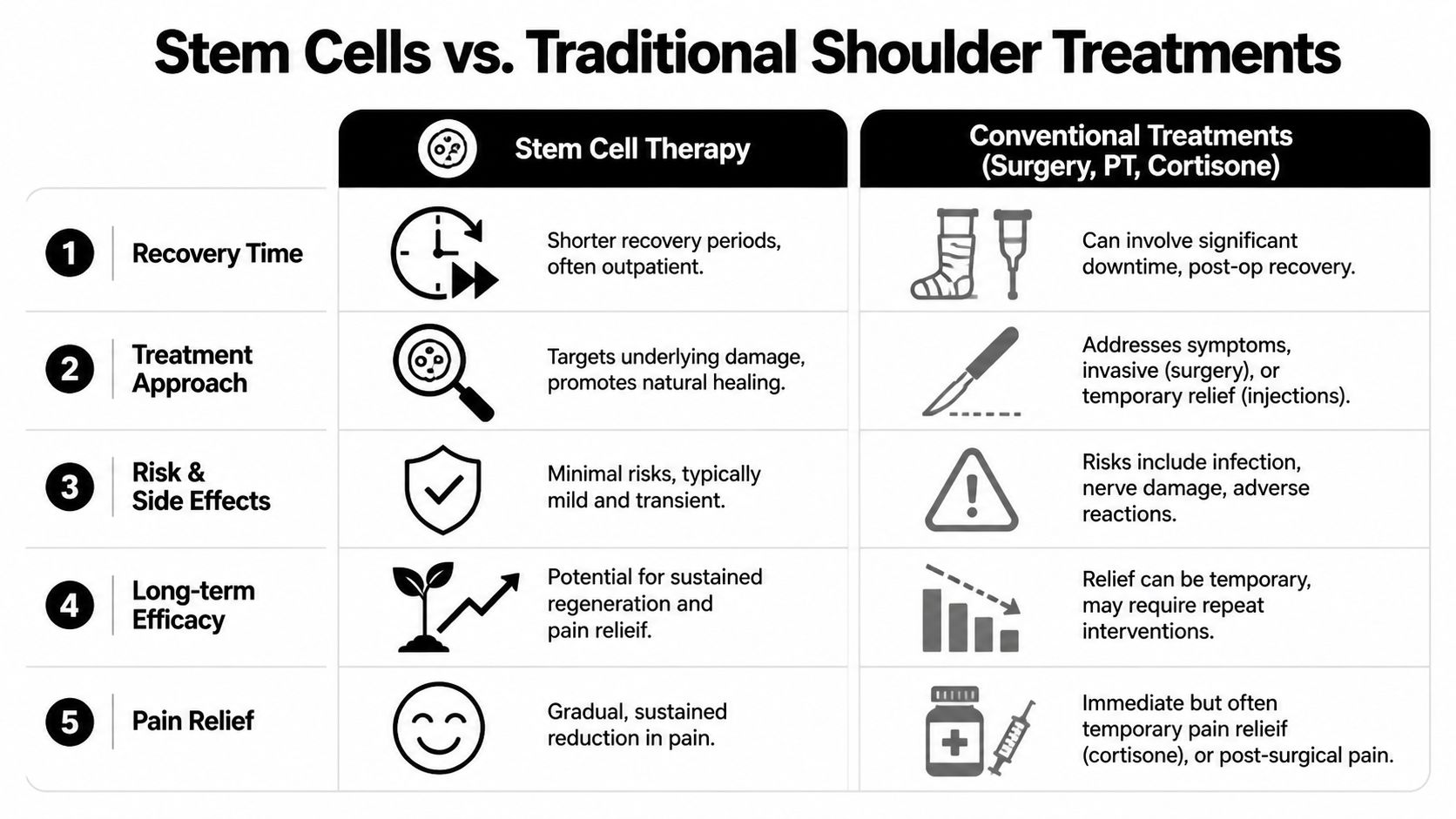
| Treatment | Mechanism | Recovery Time | Typical Outcome |
|---|---|---|---|
| Stem cell therapy | Aims to improve the tissue environment, support repair signaling, and modulate inflammation | Usually outpatient, with staged recovery over weeks to months | May improve pain, function, and tissue quality in selected cases |
| Cortisone injection | Reduces inflammatory symptoms | Usually quick short-term recovery | Often temporary relief with limited restorative effect |
| PRP | Delivers concentrated platelet-derived growth factors | Usually outpatient | Can help selected cases, especially milder injuries or adjunctive care |
| Surgery | Mechanically repairs, reconstructs, or removes damaged tissue | Typically longer rehabilitation | Can be necessary in structural cases, but recovery is more extensive and failure risk is significant |
| Physical therapy alone | Improves mechanics, strength, and movement patterns | Ongoing | Valuable foundation, though biologically compromised tissue may continue to limit progress |
How these choices work in practice
The strongest treatment plans are rarely one-dimensional. Physical therapy may be the starting point. A biologic procedure may create a better healing environment so therapy can finally gain traction. Surgery may still be the correct answer, followed by targeted regenerative support and disciplined rehabilitation.
That is also why clinic selection matters. Many centers offer only one procedure and try to fit every shoulder into it. Our model is narrower in one sense and broader in another. We use premium allogeneic stem cell protocols when the case justifies them, but we place that treatment inside a larger physician-led plan that includes diagnostics, ultrasound-guided precision, rehab sequencing, and travel safety standards. Patients considering destination care should review the Safety of Allogeneic Mesenchymal Stromal Cell Therapy Across Human Clinical Indications: A Systematic Review of Landmark Clinical Trials and Published Safety Evidence before committing anywhere.
For the right patient, stem cell therapy for shoulder injuries can offer a less invasive path than surgery with a different goal. Surgery changes structure mechanically. Regenerative medicine aims to improve how damaged tissue behaves, heals, and tolerates load over time.
Planning Your Treatment Journey to Los Cabos
Traveling for medical care is a serious decision. Patients from the U.S. and Canada usually want three things before they commit. They want to understand whether they’re a candidate, what the experience will look like on the ground, and whether the clinic has systems that make the process feel organized rather than improvised.
That process should start remotely. A proper virtual review helps determine whether your imaging, symptoms, and goals fit a regenerative pathway before you book travel. If the case appears appropriate, the next steps usually include records review, scheduling, travel coordination, and planning enough time on site for evaluation, treatment, and immediate follow-up.
For people evaluating destination care, this guide to safe stem cell therapy in Los Cabos outlines the practical safety questions worth asking before any trip.
What value means in this setting
Value isn't lower cost or convenience. It’s access to a physician-led protocol, high-level diagnostics, lab oversight, image-guided treatment, and coordinated aftercare in one setting. For many patients, that combination is what makes medical travel rational.
A well-run experience should also account for logistics. That includes clear scheduling, accommodation support, airport coordination when needed, and realistic post-procedure instructions so the trip feels calm instead of complicated.
Frequently Asked Questions About Shoulder Therapy
How many treatments do people usually need
It depends on the diagnosis, tissue quality, and how long the problem has been present. Some shoulders are treated with a single focused procedure, while more complex cases may need a staged plan or adjunctive therapies.
Does the injection hurt
Most patients describe it as very tolerable. The key difference is that this is an ultrasound-guided procedure, so the physician is targeting the tissue with precision rather than probing blindly.
Can older injuries still respond
Yes, some can. Chronic injuries often have more degeneration and compensation patterns, so the treatment plan has to be more thoughtful. Older does not automatically mean untreatable, but it does require honest expectations.
Is this only for athletes
No. Athletes often seek it because they notice performance loss early, but many ideal candidates are active adults who want to sleep better, move comfortably, and avoid a bigger intervention.
Can shoulder treatment be part of a broader longevity plan
Yes. In many patients, orthopedic recovery improves when sleep, inflammation, metabolic health, and recovery capacity are addressed alongside the local shoulder problem.
If you're considering Longevity Medical Institute for stem cell therapy for shoulder injuries, the next step is a consultation built around diagnostic clarity, candidacy, and a realistic treatment plan. Patients who travel for care usually do best when they start with a records review and a focused discussion of goals, imaging, and prior treatment history.
Author: Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review: Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: May 3, 2026
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.