A Clinical Guide to Molecular Hydrogen Therapy
Hydrogen is often considered simple. It's part of water, part of basic chemistry, and easy to overlook. But how can the smallest molecule in the body's environment become clinically relevant in recovery, inflammation, and longevity medicine?
That question exposes a gap in conventional thinking. Many patients are taught to think only in terms of drugs, supplements, or surgery. But medicine also uses gases. Oxygen is the obvious example. Nitric oxide is another. Molecular hydrogen therapy belongs in that same conversation, not as a miracle claim, but as a carefully studied tool with growing clinical interest.
In practice, patients are often surprised that hydrogen isn't being discussed as “just water.” It is molecular hydrogen, H₂, used on its own in forms such as inhalation, hydrogen-rich water, and hydrogen-rich saline. In a modern regenerative setting, that matters because the goal isn't merely to add another wellness product. The goal is to influence the biologic environment in a precise, low-burden way that may support recovery, resilience, and cellular balance.
At a clinical level, this fits into a broader philosophy of regeneration. If you'd like a wider view of that framework, our overview of the power of regeneration is a helpful starting point.
An Introduction to Hydrogen Therapy
Why would a clinician add the smallest molecule in nature to a longevity program built around far more visible interventions?
The answer starts with a simple clinical reality. Many patients arrive with fatigue, slower recovery, or signs of persistent inflammatory strain after they have already tightened the basics. Sleep is better. Nutrition is cleaner. Exercise is appropriate. Supplements are in place. Yet the internal biologic environment still appears stressed. In that setting, physicians often look for low-burden therapies that may help stabilize recovery rather than only adding more intensity.
Molecular hydrogen therapy uses hydrogen gas, H₂, in medical and wellness settings to support the body's handling of oxidative stress and inflammation. Patients often stumble over that idea because hydrogen feels too familiar to sound therapeutic. It is a bit like overlooking a master key because it is small. Size and simplicity do not determine biologic relevance. Distribution, selectivity, and interaction with cellular chemistry do.
Interest in hydrogen therapy grew after early laboratory work suggested that hydrogen could interact with damaging reactive species in a selective way. From there, the field expanded into preclinical and human research, and into practical delivery methods such as inhalation, hydrogen-rich water, and hydrogen-rich saline. That progression matters because it moved hydrogen from a chemistry curiosity into a clinical discussion.
Why patients find this confusing
Two misunderstandings create most of the confusion.
Hydrogen sounds like “just water” or basic chemistry. In clinical use, the focus is molecular hydrogen itself, delivered in ways that allow it to circulate and interact with tissues.
Online discussions often flatten the nuance. Some sources dismiss hydrogen before examining the biology. Others present it as if one intervention could solve every problem in medicine.
A more accurate frame is this: hydrogen functions as a supportive tool within a treatment plan. Clinicians use it to improve the physiologic setting in which healing and adaptation occur.
Where it fits in a longevity setting
In an advanced longevity practice, hydrogen is rarely considered in isolation. It is more often layered into a broader protocol that may include hyperbaric oxygen therapy, regenerative orthopedics, stem cell procedures, peptide-based strategies, or structured recovery programming. The goal is straightforward. Reduce unnecessary biologic friction while the body is being asked to repair, adapt, and rebuild.
That integrated view is what makes hydrogen interesting in clinical medicine. A gardener does not strengthen a plant only by changing the seed. The soil, water, light, and timing also shape the outcome. Hydrogen occupies a similar role. It may help improve the physiologic terrain so other therapies can be delivered under better conditions, especially in patients dealing with inflammation, oxidative burden, or slow recovery. For a broader explanation of that treatment philosophy, see our overview of regenerative medicine and the power of regeneration.
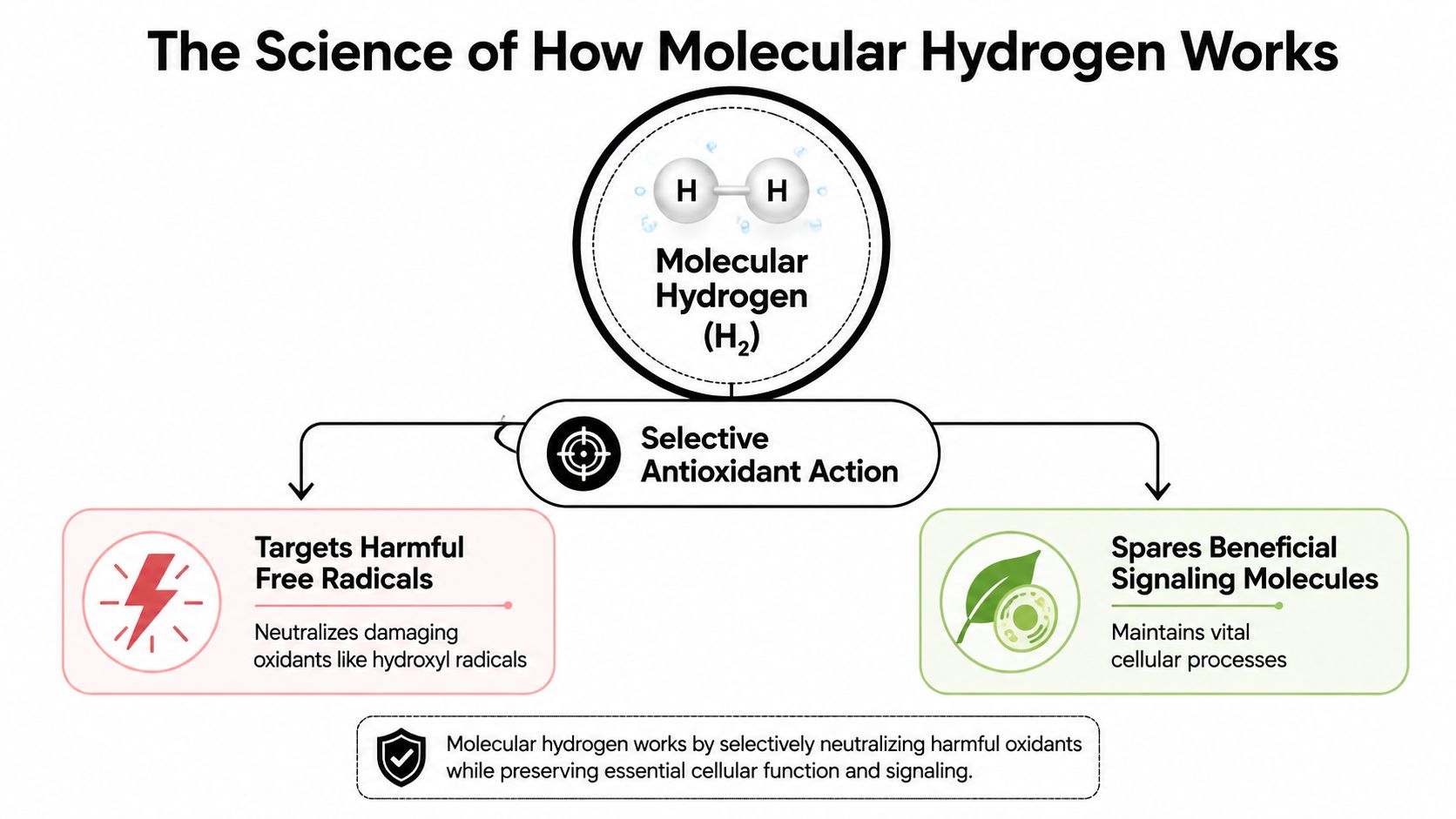
The Science of How Molecular Hydrogen Works
Why would a gas as small and simple as hydrogen matter in medicine at all?
The answer starts with scale. Molecular hydrogen is the smallest molecule in nature, which gives it unusual access to biologic spaces where larger compounds may move less freely. That does not make it magical. It makes it clinically interesting, especially in settings where physicians are trying to reduce oxidative burden without disturbing the signaling the body still needs for repair and adaptation.
Cells continuously generate reactive molecules. Some are useful. They act like text messages between cells, helping regulate immunity, energy production, and recovery. Others are far more destructive. When those aggressive species build up beyond the body's ability to control them, they can injure membranes, proteins, and DNA. That state is what clinicians call oxidative stress.
Clinical reviews describe molecular hydrogen as a selective antioxidant because it can neutralize highly reactive species such as hydroxyl radicals while preserving other redox signals. That distinction matters. Redox signaling is part of normal physiology, so a therapy that supports balance without broadly suppressing signaling is more attractive in clinical practice. The same review explains why inhalation, hydrogen-rich water, and hydrogen-rich saline have been studied across cardiovascular, respiratory, neurologic, and oncology settings (clinical review on selective antioxidant action and delivery routes).
The precision cleanup analogy
An analogy for this precision is a hospital cleaning team.
A poorly designed cleanup protocol strips a room of everything, including equipment clinicians still need. A well-designed protocol removes the hazardous contamination while leaving the tools for patient care in place. Molecular hydrogen is being studied through a similar lens. Researchers are interested in its ability to target especially damaging oxidants while allowing useful cellular communication to continue.
That selective behavior is one reason hydrogen keeps appearing in longevity and regenerative medicine conversations.
Why that matters for inflammation and aging
Oxidative stress rarely acts alone. It often feeds inflammation, and inflammation can drive further oxidative stress in return. Over time, that loop can create the pattern many patients recognize long before they have language for it. Recovery slows. Exercise tolerance drops. Tissue irritation lingers. Resilience becomes less reliable.
Hydrogen is relevant here because clinicians are often trying to lower background biologic stress, not merely mute symptoms. In a longevity program, that distinction matters. The goal is to create better conditions for healing, adaptation, and response to other therapies.
This is also why hydrogen makes more sense as part of an integrated protocol than as a stand-alone solution. For example, a patient receiving hyperbaric oxygen therapy for tissue repair and recovery support may also benefit from strategies that help manage oxidative load during treatment cycles. In that context, hydrogen is better understood as a supporting tool within regenerative care, alongside interventions such as HBOT, peptides, or cell-based therapies.
Clinical lens: A therapy does not need to behave like a conventional drug to be useful. The practical question is whether it improves the physiologic environment in a measurable way.
Why route matters scientifically
Mechanism also depends on delivery. Hydrogen therapy is not one uniform exposure. Inhalation, hydrogen-rich water, and hydrogen-rich saline produce different concentration patterns, different timing, and different levels of systemic exposure.
That matters in real clinical planning. A physician considering hydrogen for short-term procedural support may think differently than one using it for lower-intensity, repeated exposure over time. The science becomes much easier to understand once you view hydrogen less as a single product and more as a tool whose effects depend on dose, route, and the larger treatment strategy around it.
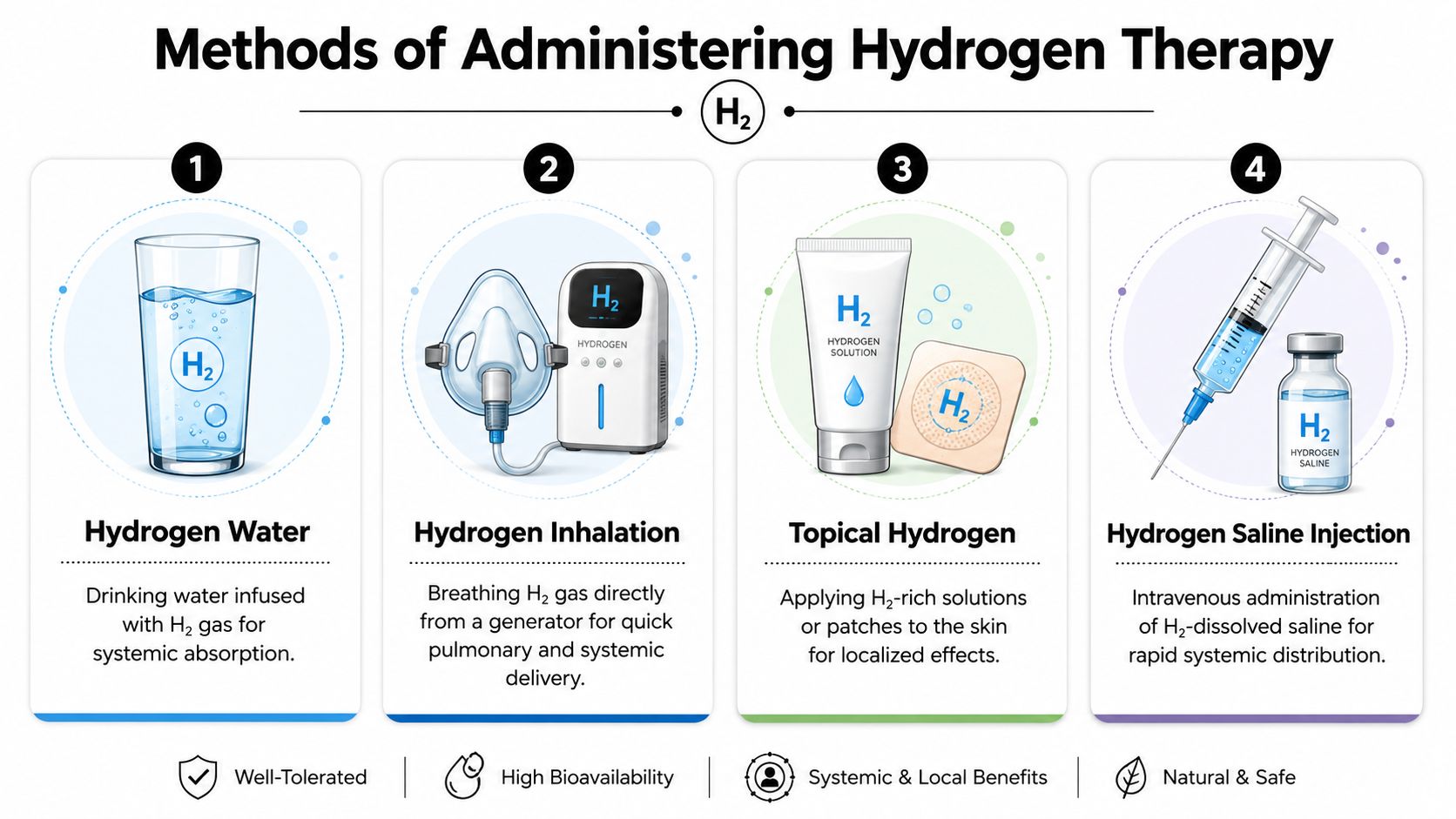
Methods of Administering Hydrogen Therapy
When patients hear “hydrogen therapy,” they often imagine one device and one protocol. In reality, molecular hydrogen therapy is delivered in several different ways, and each route changes the patient experience and the clinical use case.
A side by side clinical view
| Method | What the patient does | Typical role in care | Practical notes |
|---|---|---|---|
| Inhalation | Breathes hydrogen gas through a mask or nasal interface | Often used when clinicians want direct systemic delivery | Usually the most medicalized format |
| Hydrogen-rich water | Drinks water infused with dissolved H₂ | Often used for ongoing daily support | Simple and accessible, but exposure can vary |
| Hydrogen-rich saline infusion | Receives saline containing dissolved hydrogen in a clinical setting | Considered when a physician wants a supervised systemic route | Requires medical oversight |
| Topical use | Uses hydrogen-rich baths or local applications | Considered for localized comfort or adjunctive support | Less commonly discussed by patients, but still part of the platform |
Inhalation
This is the route many clinicians think of first. It's straightforward: the patient sits comfortably and breathes a controlled hydrogen mixture. In published trials, inhalation is described as the most clinically used route.
Patients usually like inhalation because it's passive. You don't need to “do” much beyond sit, breathe, and relax. In an integrated plan, it can also be paired with other supportive interventions. Some clinics incorporate it into broader recovery systems, and in some settings it may be considered alongside options such as IV therapy for inflammation when a physician is building a layered protocol.
Hydrogen-rich water
This is the easiest route to understand because it feels familiar. You drink water that contains dissolved hydrogen gas. The appeal is convenience. The limitation is that convenience and dosing precision don't always move together.
For wellness-oriented support, this route may fit patients who want a lower-intensity option. For acute or highly supervised care, many clinicians prefer more direct delivery.
Hydrogen-rich saline infusion and topical formats
Hydrogen-rich saline is generally a clinic-based intervention. It isn't a casual self-care tool. It belongs in medical hands, where route, timing, and indication are being matched to the patient.
Topical methods, including baths and localized applications, are less central in public discussion but still relevant. They remind us that hydrogen therapy isn't just one product. It's a delivery platform, and the route should match the treatment objective.
The best method isn't the one that sounds most advanced. It's the one that fits the clinical goal, the setting, and the patient's tolerance for treatment complexity.
Reviewing the Clinical Evidence
How do you judge a therapy that attracts both serious scientific interest and exaggerated online claims? The best place to start is the shape of the evidence itself.
Molecular hydrogen has moved well beyond the stage of isolated lab curiosity. The literature now includes basic science, translational research, and human studies across several medical settings. That does not settle every clinical question. It does tell us the topic deserves a careful reading rather than a dismissive one.
The arc of the research
The research story matters because it shows whether a concept can survive contact with real clinical testing. Hydrogen first drew broad attention after early work suggested it could interact with some of the most damaging reactive species in the body without shutting down the signaling molecules cells still need. That distinction helps explain why clinicians remain interested. The goal is not to silence oxidation across the board. The goal is to reduce the kind of oxidative stress that behaves more like uncontrolled electrical sparking than normal cellular communication.
Over time, the field expanded from mechanism studies into human investigations and review-level papers. Researchers have examined hydrogen in contexts that include neurologic disease, cardiometabolic stress, inflammatory conditions, exercise recovery, critical illness, and infectious disease. Some of these signals are stronger than others, but the overall pattern is clear. Hydrogen is being studied as a biologically active intervention, not as a fringe wellness idea.
What the evidence supports most clearly
A disciplined reading of the literature leads to a measured conclusion.
Hydrogen appears to have plausible mechanisms, a growing human evidence base, and enough consistency across studies to justify continued clinical use in selected settings. At the same time, the studies are often small, the protocols vary, and the treatment methods are not always comparable. Drinking hydrogen-rich water, inhaling hydrogen gas, and using hydrogen-rich saline are not interchangeable exposures any more than a topical cream and an IV infusion would be considered the same treatment.
That variability is where patients often get confused. A headline may say hydrogen helped fatigue, inflammation, or recovery, but the actual result usually depends on route, dose, timing, and patient population. In practice, that means the question is rarely “Does hydrogen work?” A better question is “For which patient, by which method, and as part of what larger protocol?”
A clinical interpretation that holds up
At a premium longevity clinic, hydrogen is rarely framed as a stand-alone answer. It is better understood as a support tool inside a larger therapeutic strategy. In the same way that a skilled surgeon uses the right instrument for a specific step rather than one instrument for the entire procedure, longevity physicians may use molecular hydrogen to support recovery biology while other therapies address tissue repair, oxygen delivery, metabolic dysfunction, or immune regulation.
This is why hydrogen becomes more interesting, not less, in advanced care. Its value may be highest when it is paired thoughtfully with regenerative medicine, hyperbaric oxygen therapy, structured rehabilitation, or targeted infusion protocols. In that setting, the clinical goal is not hype. The clinical goal is better tolerance, better recovery, and a more favorable physiologic environment for other interventions to work.
Patients should also expect honest limits. The current literature supports cautious optimism, selective use, and ongoing study. It does not justify sweeping disease claims. It does not replace diagnosis. It does not remove the need for physician oversight, especially when hydrogen is being added to an already advanced treatment plan. Our standard for integrating therapies is the same standard described in our guide to safety and transparency in clinical decision-making.
What matters most: the evidence supports molecular hydrogen as a credible adjunct in medicine and longevity care, especially when it is integrated with other regenerative strategies. It should be presented as a tool with defined strengths, not as a cure-all.
Safety Dosing and Patient Guidance
When people first hear about molecular hydrogen therapy, safety is usually the first practical concern. That's appropriate. In longevity medicine, novelty alone does not make a therapy attractive. It has to be usable, tolerable, and rational in real patients.
A key fact from research summaries is that hydrogen is used at very low concentrations while still remaining biologically active. A saturated hydrogen solution contains about 1.6 parts per million (ppm) H₂, while inhalation protocols commonly use 1–3% hydrogen gas. The same summary also notes that hydrogen has been investigated for multiple endpoints, including improved symptoms in rheumatoid arthritis and Parkinson's disease and reductions in exercise-related fatigue (clinical safety and delivery overview from the Alzheimer's Drug Discovery Foundation).
What patients should understand about dosing
Dosing in hydrogen therapy doesn't work like a standard prescription where one number fits everyone. Clinicians think in terms of:
Route of delivery
Treatment context
Frequency of exposure
Whether the goal is acute support or longer-term adjunctive care
This is one reason self-experimentation can become confusing. A patient may compare hydrogen water, home devices, and clinic protocols as if they were interchangeable. They aren't.
Practical safety guidance
For most patients, the key questions are simple.
Am I using the right form for my goal? Inhalation, water, and infusion are not the same intervention.
Is this medically supervised? That matters more when hydrogen is being integrated with other therapies or used in a more complex medical context.
Am I expecting too much from one tool? Hydrogen may support outcomes, but it shouldn't be treated as a replacement for diagnosis, medication review, or foundational care.
A careful clinic will also look at the broader safety picture. That includes your diagnoses, your medications, your symptom pattern, and the logic of combining therapies. Patients who value that kind of process usually appreciate our approach to safety and transparency.
What I tell patients in plain language
Hydrogen is appealing partly because the exposure levels used are low and the therapy is generally discussed as having a favorable safety profile. But “favorable” doesn't mean casual. It means the therapy should be matched to the person.
If you're medically complex, the right question isn't “Is hydrogen safe in general?” It's “Is this the right route, timing, and setting for me?”
That mindset protects patients from two extremes. One is unnecessary fear. The other is overconfidence.
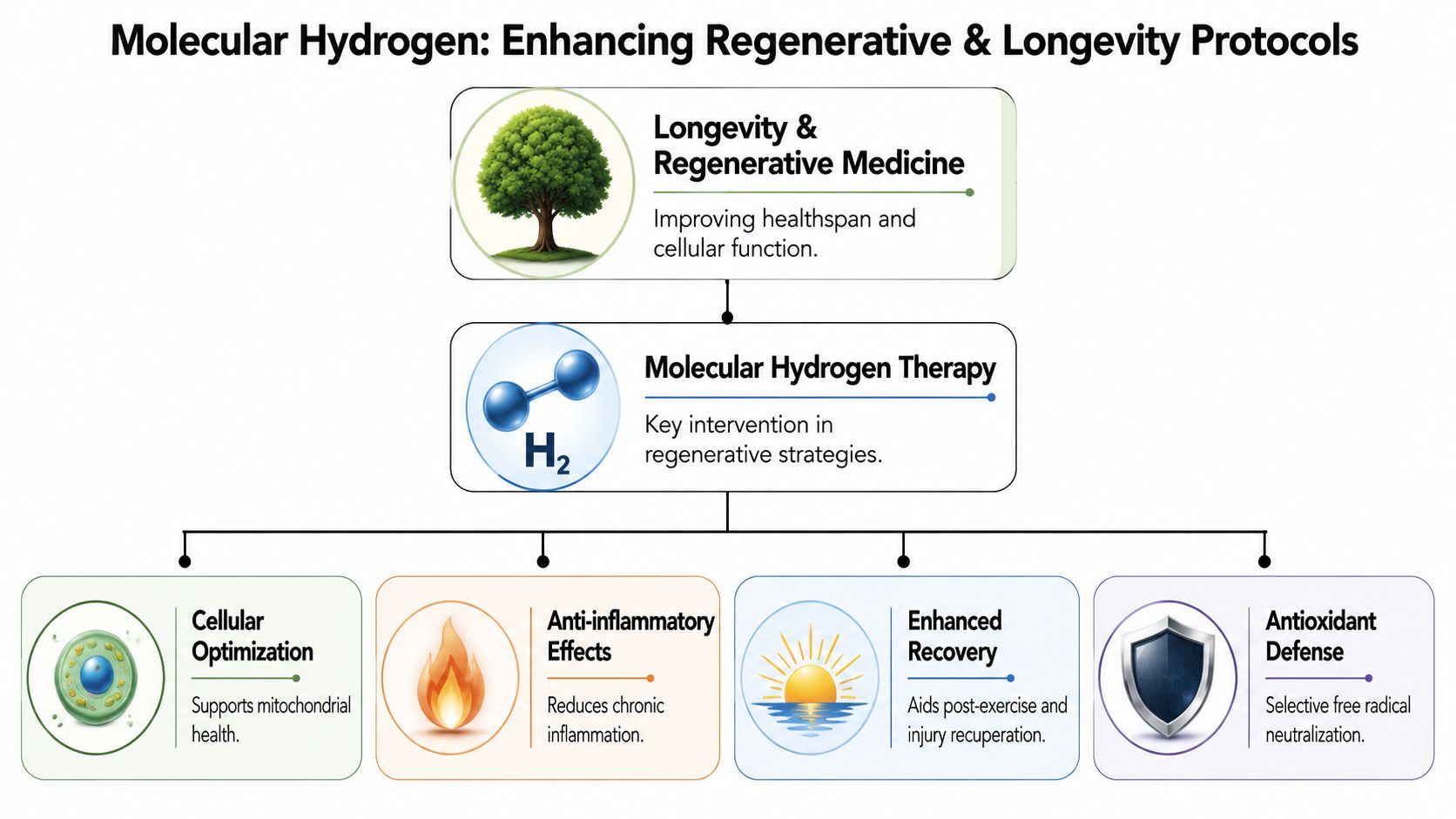
Enhancing Regenerative and Longevity Protocols
Where does molecular hydrogen belong in a serious longevity program?
In clinical practice, its value usually appears in the way it supports the treatment setting around other interventions. Molecular hydrogen is best placed as a supportive biologic tool within a broader regenerative plan, especially when the goal is to improve recovery conditions, reduce physiologic stress, and help patients tolerate layered care more effectively.
Why integration matters
Regenerative medicine is rarely a single intervention. A patient may be receiving allogeneic cell therapy, peptide support, oxygen-based care, IV therapies, or light-based recovery work, yet all of those inputs still act within the same internal terrain. If that terrain is marked by oxidative stress, poor recovery, or persistent inflammatory signaling, the overall program can become harder for the body to use well.
That is why clinicians pay attention to the treatment environment, not just the headline therapy.
Hydrogen becomes clinically interesting at this level. It may help create conditions that are more favorable for recovery-focused and regenerative therapies, which is one reason it is often considered as part of an integrated protocol rather than as an isolated intervention.
Where it may fit alongside other therapies
The practical question is not whether hydrogen stands above other modalities. The practical question is where it fits most logically.
With allogeneic stem cell programs. At our institute, regenerative care may involve allogeneic cell sources including placental, Wharton's jelly, adipose, endometrial, and dental pulp. In that setting, hydrogen may be used to support a less oxidatively burdened internal environment while the larger care plan is underway.
With hyperbaric or oxygen-based care. Some patients benefit from protocols that combine oxygen-focused therapies with recovery support, particularly when timing, sequence, and supervision are carefully matched to the patient.
With peptide and recovery protocols. Hydrogen may suit patients who are dealing with training load, travel stress, post-procedural recovery, or lower physiologic reserve.
With light-based modalities. Treatments such as photobiomodulation therapy target repair and recovery through different biologic pathways. Hydrogen may be added when the clinical aim is to support that work from another angle.
A systems-based way to think about hydrogen
A useful comparison is perioperative optimization. In surgery, the procedure matters, but so do oxygenation, inflammation control, and recovery capacity because they influence how well the patient comes through the process. Regenerative medicine follows a similar logic. The therapy may be the main intervention, yet the surrounding biology still shapes the result.
Hydrogen fits into that surrounding biology.
This perspective matters in longevity care because patients rarely present with one clean, isolated issue. More often, they arrive with layered concerns such as slower recovery, disrupted sleep, inflammatory symptoms, reduced exercise tolerance, and age-related loss of resilience. In that context, a therapy does not need to dominate the protocol to be useful. It needs to improve how the whole plan functions.
One example is the use of molecular hydrogen inhalation within a multi-modality regenerative station. Longevity Medical Institute includes molecular hydrogen inhalation as one component of a 5-in-1 regenerative therapy station, alongside other complementary recovery inputs, so physicians can place hydrogen within a broader therapeutic sequence rather than treating it as a stand-alone claim.
In integrated care, the better question is often simple. Does this therapy improve the physiologic conditions in which the rest of the plan is being delivered? For molecular hydrogen, that is often the most clinically relevant question.
Frequently Asked Questions About Hydrogen Therapy
What does treatment feel like
Most patients find hydrogen inhalation easy to tolerate. It typically feels like sitting and breathing through a comfortable interface. Hydrogen-rich water feels no different from drinking ordinary water, which is one reason patients sometimes underestimate that it's a real intervention.
How soon might I notice an effect
That depends on why you're using it. Some people report that recovery-oriented therapies feel subjectively calming or supportive early on. Others notice nothing dramatic and only appreciate changes over time within a larger plan. That's normal. Molecular hydrogen therapy is usually better judged by context than by a dramatic immediate sensation.
Is this a stand-alone treatment
Usually, no. In serious clinical practice, hydrogen makes the most sense as part of a broader strategy. It may complement work on inflammation, recovery, resilience, and regenerative support, but it shouldn't replace proper evaluation.
Can I use it with my current medications
Possibly, but that decision belongs with your treating clinician. The main issue isn't that hydrogen is commonly framed as highly interactive. The main issue is that your full medical picture matters. If you're taking medications, especially for chronic or complex conditions, coordination is the safe approach.
Is inhalation better than hydrogen water
Not automatically. Inhalation is often chosen when clinicians want a more direct delivery route. Hydrogen-rich water may be attractive for routine use because it is simpler. “Better” depends on the goal, the patient, and the level of supervision needed.
Who should ask more questions before starting
Anyone with a complicated diagnosis, active medical treatment, or a tendency to self-layer multiple wellness interventions without oversight. Hydrogen may be low burden, but low burden is not the same as no need for clinical judgment.
Why do premium clinics use it differently than wellness brands
Because a clinical team looks at sequence, indication, route, and integration. A wellness brand may sell a product. A physician-led program asks a different question: where does this fit, and what is it meant to support?
If you're exploring molecular hydrogen therapy as part of a broader recovery, regenerative, or longevity strategy, a physician-guided plan matters. To learn how this therapy may fit within a personalized program, visit Longevity Medical Institute.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: June 15, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.