Prostate MRI: Your Guide to Understanding Results
A rising PSA often creates a very specific kind of stress. You're told something may be wrong, but you still don't know what the result means, whether cancer is present, or whether the next step has to be a biopsy.
For years, that uncertainty pushed many men into a familiar pattern. Repeat blood tests. Worry. A biopsy that sampled the prostate in a systematic but imperfect way. Then more waiting. Modern prostate imaging has changed that sequence. A prostate MRI gives doctors a far more detailed map before any needle is used, and that changes the quality of every decision that follows.
For patients, that matters because clarity is its own form of treatment. A good diagnostic test doesn't just detect disease. It reduces guesswork, avoids unnecessary procedures, and turns a vague threat into something visible, measurable, and actionable.
Navigating Prostate Health in an Era of Precision
A common scenario starts with a routine physical. A man feels well, has no major urinary symptoms, and then gets a message through the patient portal that his PSA is high or rising. The number itself doesn't diagnose cancer, but it immediately changes the emotional temperature of the week.
The old pathway often felt blunt. If concern remained high, many men moved toward biopsy without first seeing where the problem might be. That approach can find cancer, but it can also miss important disease or identify low-risk findings that create more anxiety than value.
Why the diagnostic pathway has changed
Pre-biopsy MRI has moved from a niche tool to a standard part of modern prostate evaluation. Its use increased from 0.5% in 2014 to 35% in 2024, a 70-fold increase, and evidence reviewed by the Prostate Cancer Foundation notes that MRI-informed decisions could have avoided 38% of biopsies while still identifying 89% of clinically significant cancers in the cited study population (Prostate Cancer Foundation patient guide).
That shift reflects something patients immediately understand. If a scan can help show who needs tissue sampling and who may safely avoid it, the entire process becomes more rational.
For men thinking broadly about prevention while they sort through prostate questions, practical lifestyle support still matters.
Precision creates leverage
A prostate MRI works like a high-resolution navigation system. Instead of driving through fog with only a rough paper map, your physician can see suspicious regions, assess whether the gland looks reassuring or concerning, and decide whether biopsy is necessary at all.
A better test doesn't remove every difficult decision. It improves the quality of the decision you make.
That's the core value. Men gain a more informed conversation with their physician, and doctors gain a more precise tool for triage. If you're evaluating where to start, structured programs in urology and men's health care can help place MRI findings in the broader context of PSA trends, symptoms, family history, and long-term planning.
What Is a Multiparametric Prostate MRI
Multiparametric MRI, often called mpMRI, is more than a picture of the prostate. It's a layered analysis of anatomy and tissue behavior. Think of it as combining a street map, a weather radar image, and a heat signature into one integrated view of the same area.
That's why “multiparametric” matters. A single image can show shape. Several coordinated image types can show shape, density, and vascular behavior at the same time.
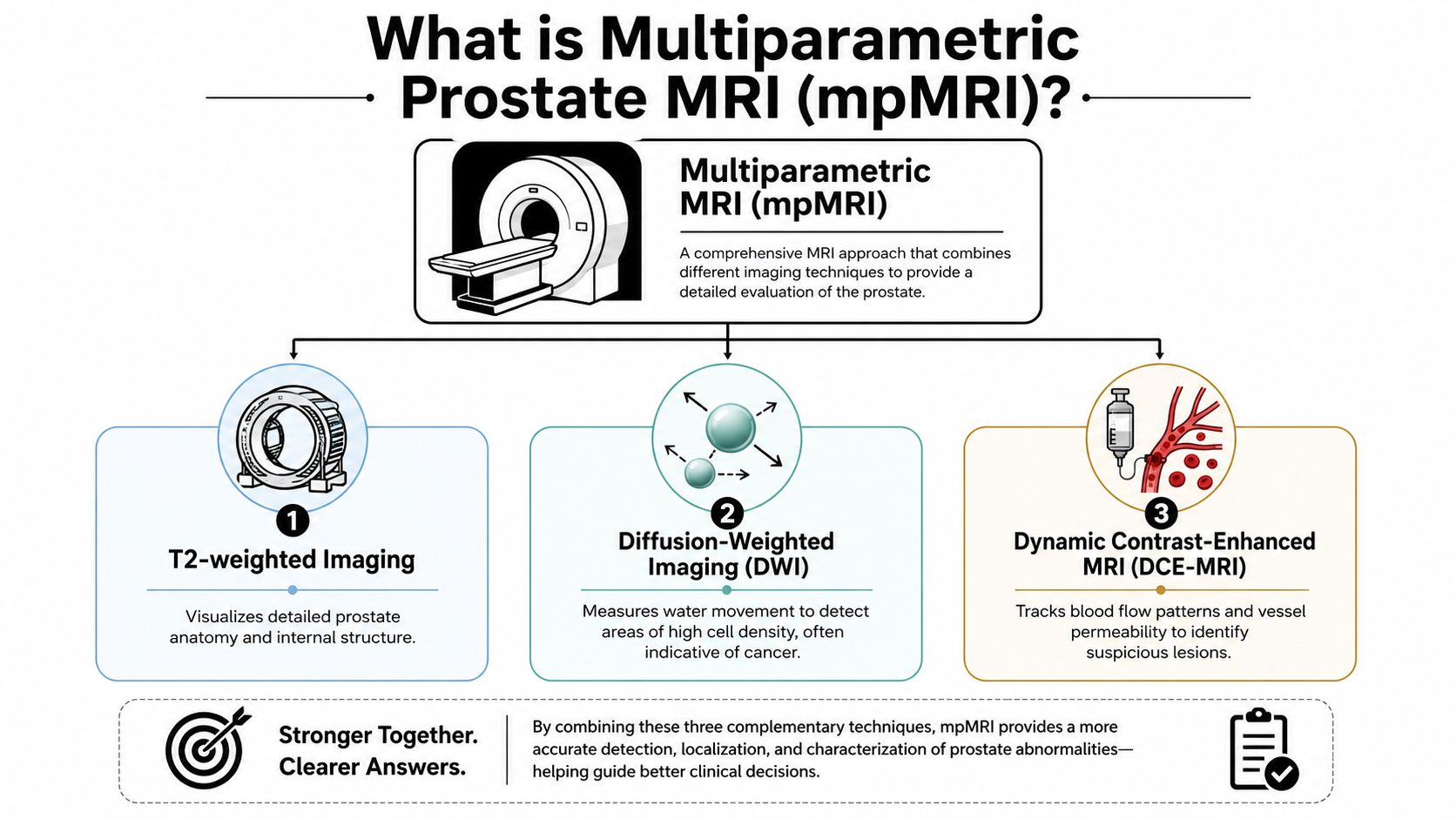
The three core views radiologists use
A diagnostic prostate MRI typically includes T1 and T2-weighted sequences for morphology, diffusion-weighted imaging (DWI), and dynamic contrast enhancement (DCE). The protocol also requires axial oblique images with slice thickness of ≤3 mm for high-definition visualization (Radiopaedia prostate MRI protocol).
In practical terms, each part contributes something different:
T2-weighted imaging shows the prostate's internal structure and zonal anatomy in fine detail.
Diffusion-weighted imaging looks at water motion inside tissue. Areas with dense, abnormal cells often restrict that motion.
Dynamic contrast-enhanced imaging observes how tissue takes up contrast, which can help highlight suspicious vascular patterns.
T1-weighted imaging helps with broader structural assessment and can identify findings such as hemorrhage after prior procedures.
Why this is different from a simple scan
A standard image gives a snapshot. mpMRI gives context. If one sequence raises concern but the others don't support it, that changes interpretation. If multiple parameters point to the same lesion, confidence rises.
This layered method is one reason experienced centers can identify suspicious targets more intelligently than older imaging pathways. It's also why image quality and protocol discipline matter so much. A poorly executed MRI isn't just less elegant. It can be clinically misleading.
Clinical perspective: The value of mpMRI comes from the combination of sequences, not from any single image in isolation.
Patients who've already explored advanced imaging in other parts of medicine often recognize the same principle in AI-supported full body MRI. Better imaging isn't about producing more pictures. It's about generating a more useful map.
When Is a Prostate MRI Recommended
Doctors don't order a prostate MRI for its advanced capabilities alone. They order it when the result is likely to change management. That usually means there is a real question to answer, and MRI can sharpen the answer before anyone commits to an invasive step.
The most common situations
A prostate MRI is often recommended in the following settings:
After a high or rising PSA when the next step isn't obvious and biopsy is being considered.
Before a first biopsy to identify whether a suspicious lesion is present and where it is located.
After a prior negative biopsy if concern remains because PSA continues to rise or the broader clinical picture still feels unsettled.
During active surveillance for men already known to have lower-risk prostate cancer and being monitored over time.
Another important use is in men with higher baseline risk, especially when personal history, family history, or race changes the threshold for early evaluation.
Who may be considered for screening MRI
The PRISM consensus recommends MRI screening for men aged 50 to 70 with a life expectancy exceeding 10 years, and advises starting at age 45 for Black men because of higher risk profiles (PRISM consensus on PubMed).
That doesn't mean every man in that age range needs the same pathway. It means risk should be stratified rather than handled with a one-size-fits-all script.
The decision is rarely based on one number
A thoughtful recommendation usually blends several factors:
PSA pattern over time, not just one isolated result.
Exam findings if a digital rectal exam raises concern.
Personal and family risk including ancestry and prior history.
Previous biopsy history and whether suspicion remains unresolved.
For patients who need procedural planning after imaging or abnormal findings, resources on advanced urology procedures can help clarify what comes after the MRI and why the sequence of care matters.
Understanding Your PI-RADS Score
Once the MRI is complete, the report usually centers on one framework: PI-RADS. This stands for Prostate Imaging Reporting and Data System, and it assigns a score from 1 to 5 to estimate how likely a lesion is to represent clinically significant prostate cancer (Mayo Clinic overview of prostate MRI and PI-RADS).
That score doesn't diagnose cancer by itself. It organizes risk so the next step makes sense.

What the numbers mean
| PI-RADS score | What it generally suggests | Typical clinical direction |
|---|---|---|
| 1 | Very low likelihood of clinically significant cancer | Usually reassurance, monitoring as appropriate |
| 2 | Low likelihood | Often continued observation rather than immediate biopsy |
| 3 | Intermediate or indeterminate likelihood | Decision depends on PSA, history, exam, and patient factors |
| 4 | High likelihood | Targeted biopsy is commonly considered |
| 5 | Very high likelihood | Strong concern, biopsy planning usually follows |
How to read the report without overreacting
The most helpful way to think about PI-RADS is that it ranks suspicion, not certainty.
Scores 1 and 2 are generally reassuring.
Score 3 is the gray zone. It means the radiologist sees something that isn't comfortably dismissed but isn't clearly high-risk.
Scores 4 and 5 usually justify a more direct tissue diagnosis.
A high score still needs biopsy confirmation. A low score still needs to be interpreted in the context of your PSA trend and overall risk profile.
Practical rule: Don't read the score as a verdict. Read it as guidance for the next decision.
That distinction lowers anxiety and improves conversations. Patients who want a clearer framework for interpreting reports often benefit from plain-language tools such as your MRI results explained more clearly, especially before meeting with a urologist.
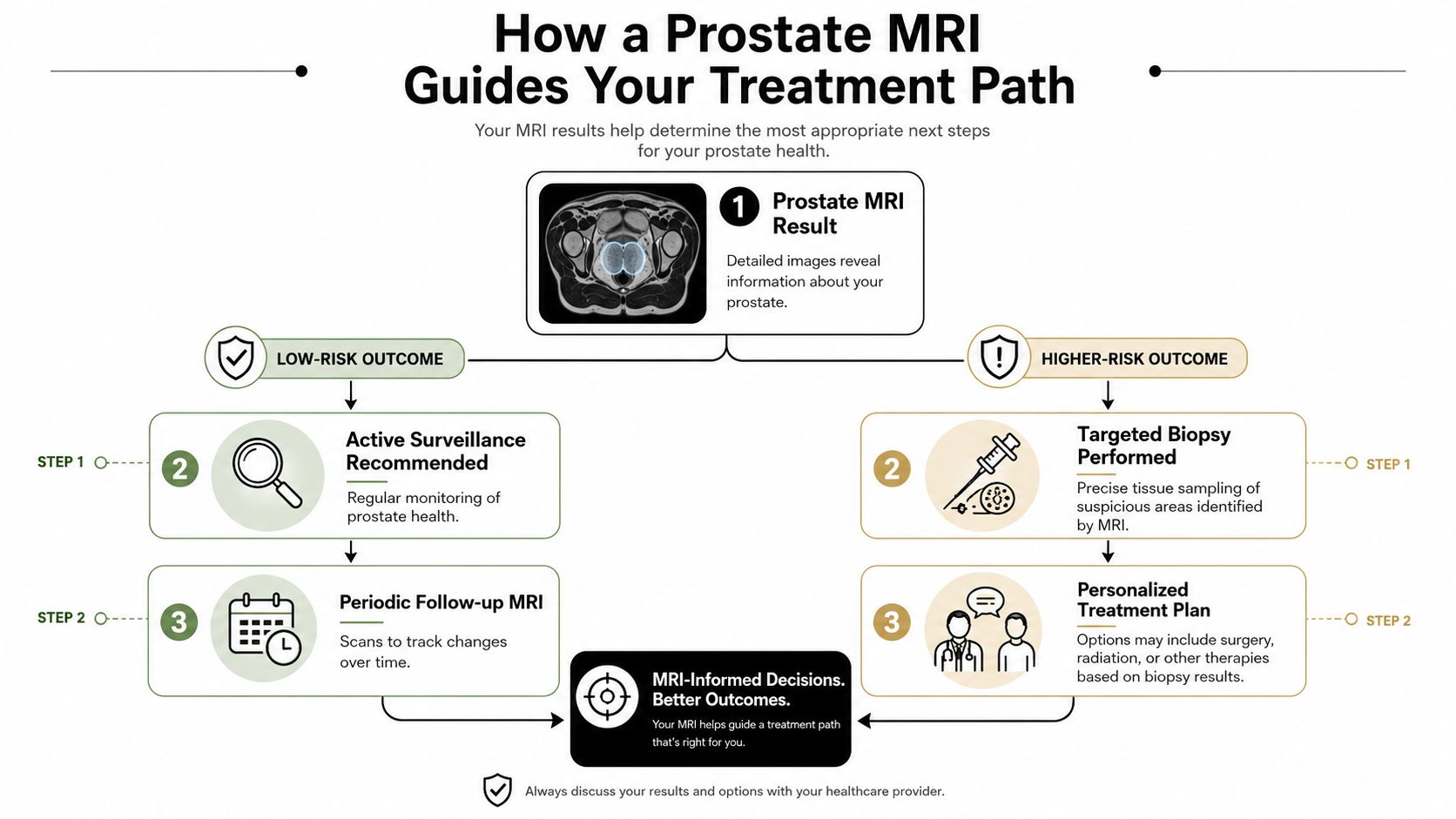
How a Prostate MRI Guides Your Treatment Path
The most important question after a prostate MRI isn't “What did the scan show?” It's “How does this change what happens next?”
That's where MRI has had the biggest impact. It separates men who need precise tissue confirmation from men who may be able to avoid biopsy and continue careful follow-up.
The old way compared with the newer pathway
Traditional transrectal ultrasound-guided biopsy sampled the gland systematically. It was useful, but in many cases it functioned like taking random soil samples from a field and hoping the core hits the exact patch where the problem sits.
MRI-guided planning changes that.
In a landmark study of 2,582 patients, using MRI before biopsy improved detection of clinically significant prostate cancer by 57% and reduced the total number of biopsy procedures by 33%. In some cohorts, MRI correctly diagnosed 93% of tumors, while standard biopsy correctly diagnosed 48% (AJR review and cited data).
When MRI points toward biopsy
If the MRI shows a suspicious lesion, the next step is often a targeted biopsy. In many settings this is performed as an MRI-ultrasound fusion biopsy, where MRI findings are overlaid with live ultrasound so the physician can direct the needle toward the exact area of concern.
That matters because:
The target is defined rather than guessed.
Sampling is more strategic because the lesion has already been localized.
Clinically important disease is less likely to be missed than with blind systematic sampling alone.
When MRI supports watchful restraint
A reassuring MRI can be just as valuable as a suspicious one. mpMRI has shown a negative predictive value ranging from 0.65 to 0.94, and one source notes a diagnostic sensitivity range of 44% to 87% with negative predictive value of 63% to 98% for clinically significant disease, helping rule out major pathology in many men (American Urological Association clinical guidance).
MRI becomes a gatekeeper. If the scan is low suspicion and the overall clinical picture fits, many men can avoid an immediate biopsy and move into surveillance instead of invasive testing.
A negative or low-suspicion MRI doesn't mean “ignore the prostate.” It means the next step may be monitoring rather than puncturing tissue today.
That is precision medicine in a very practical form. It doesn't push every patient toward intervention. It helps match the intervention to the evidence in front of you.
Preparing for Your Prostate MRI Procedure
The procedure itself is usually far less dramatic than patients expect. Most of the anxiety comes from not knowing the sequence. Once you know the rhythm of the day, the scan feels much more manageable.
Before the appointment
Your imaging center will give specific instructions, and those matter because protocol details affect image quality. Some centers ask you to adjust meals beforehand, and some may recommend simple bowel preparation so the prostate is easier to visualize clearly.
Bring a current medication list and be prepared to answer questions about:
Metal implants or devices such as pacemakers, clips, or certain older hardware
Kidney history if contrast is being considered
Prior prostate procedures because recent biopsy can affect image interpretation
Claustrophobia or anxiety so the team can plan appropriately
During the scan
You'll lie still on the MRI table while the machine acquires a series of images. The study is noisy, so ear protection is typically provided. Remaining still matters because movement blurs the anatomy and can reduce confidence in the final report.
Some scans include intravenous contrast for the dynamic contrast-enhanced portion. If contrast is used, it's there to help radiologists evaluate how tissue behaves over time, not because something is automatically wrong.
A few centers may still discuss an endorectal coil in selected cases, though many modern prostate MRI exams are performed without one. Whether that's necessary depends on the scanner, protocol, and the imaging team's preferences.
After the scan
Most patients return to normal activity right away. There's usually no recovery period. The next step is interpretation by a radiologist who reads prostate MRI regularly and reports the findings in a structured way.
If you've already reviewed broader MRI logistics, the patient experience is similar to other advanced studies described in guides on what to expect during a full body MRI. The body region changes. The importance of preparation, stillness, and expert interpretation doesn't.
Choosing a World-Class Diagnostic Center
Not every prostate MRI is equal. That statement is uncomfortable, but it's clinically important. A prostate MRI is only as good as the scanner, the protocol, and the person reading it.
What actually determines scan quality
Patients often focus on access and convenience first. Those matter, but they shouldn't outrank diagnostic quality.
Look for these features:
A disciplined prostate MRI protocol with the right sequences and technical standards.
Radiologists who read prostate MRI routinely, not only occasionally.
Clear PI-RADS reporting, so the referring doctor can act on the result.
Coordination with targeted biopsy pathways if the scan identifies a lesion.
Modern imaging infrastructure, which may include advanced software support and integrated review systems.
A high-end center doesn't help because it feels premium. It helps because the margin for interpretive error is lower when the imaging pathway is built deliberately.
Why access still isn't equal
Access remains a serious issue. Research shows that Non-Hispanic Black men are 72% less likely to receive pre-biopsy prostate MRI than White men, at 0.6% versus 2.1%, and rural patients are 35% less likely than those in large metro areas (PubMed study on disparities in pre-biopsy MRI access).
Those gaps don't exist because the technology lacks value. They reflect uneven infrastructure, referral habits, insurance barriers, and geography.
When travel for imaging makes sense
For some patients, traveling to a specialized center is the most practical way to get a definitive answer without waiting through a fragmented local process. That's especially true when the local option offers limited expertise in prostate MRI interpretation or no clear path to MRI-targeted biopsy if something suspicious appears.
One option patients sometimes consider is Longevity Medical Institute, where advanced MRI imaging is part of its men's health and diagnostic services. The broader principle is what matters most: choose a center that can deliver technical quality, expert reading, and coordinated follow-through.
If the scan result will decide whether you undergo biopsy, treatment, or surveillance, the quality of that scan is not a minor detail.
Frequently Asked Questions About Prostate MRI
Is a prostate MRI painful
Usually, no. The scan itself is noninvasive. The main discomfort is often the need to lie still in a confined space while the machine makes loud sounds.
What if I'm claustrophobic
Tell the imaging team before the appointment. Many centers can help with positioning, communication during the scan, and planning strategies to make the experience manageable. Patients do much better when the team knows about this in advance.
How long does it take to get results
Timing varies by center and by the radiologist workflow. In practice, the most important issue isn't speed alone. It's getting a careful interpretation from someone who reads prostate MRI regularly.
Is contrast dye always used
Not always. Some prostate MRI protocols include contrast, while screening-oriented abbreviated protocols may use non-contrast imaging. Your physician and the imaging center decide based on the purpose of the exam and the protocol being used.
Are there risks with the contrast dye
Contrast is commonly used when dynamic contrast-enhanced imaging is needed. The team should review kidney history and any prior contrast reactions before the exam. If there are concerns, ask directly whether contrast is necessary in your case and what alternatives exist.
Can a normal MRI completely rule out cancer
No test does that perfectly. What a good prostate MRI can do is make the next decision much smarter. In many men, a reassuring MRI supports surveillance instead of immediate biopsy, especially when the broader clinical picture is also low concern.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: July 11, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.
At Longevity Medical Institute Treatments and Resources, we are pioneers in advanced regenerative and diagnostic medicine. We exclusively use allogeneic stem cells, produced in our own state-of-the-art biotechnology lab. Our diverse cellular products include placental, Wharton's jelly, adipose, endometrial, and dental pulp-derived stem cells, allowing us to create highly personalized treatment protocols for conditions ranging from plantar fasciitis and ulcerative colitis to cognitive decline and chronic inflammation. Our integrated approach combines these therapies with a suite of advanced diagnostics and treatments available on-site, including peptides, hyperbaric oxygen therapy (HBOT), our Longevity Recharge Station, advanced sleep medicine, and extensive in-house lab testing of over 140 biomarkers. We are proud to offer leading-edge diagnostic tools such as AI-integrated Full Body Scan MRI, Advanced Heart Evaluation, and Trifusion EBOO with UV and PBM, ensuring a complete and precise picture of your health.
If you're trying to make sense of a PSA change, a prior biopsy, or a prostate MRI result, Longevity Medical Institute offers physician-led guidance that integrates advanced imaging with broader men's health evaluation, so you can move from uncertainty to a clearer plan.