Stem Cell Therapy for Crohn’s Disease: A Patient’s Guide
Living with Crohn's often means planning your day around uncertainty. You may wake up feeling almost normal, then cancel dinner by afternoon because cramping, urgency, fatigue, or bloating has taken over. Many patients tell me the hardest part isn't only the pain. It's the loss of trust in their own body.
That frustration gets sharper after you've done what you were told to do. You tried the elimination diets. You learned the medication names. You adapted your work, travel, and social life. And still, the disease keeps reminding you that symptom control isn't the same as stability.
Stem cell therapy for Crohn's disease has entered this conversation because some patients need a different strategy. Not a cosmetic upgrade to the same treatment model, but an approach aimed at immune balance, inflammatory control, and tissue repair signaling. That distinction matters. Crohn's is not just irritated bowel tissue. It's a misdirected immune process acting on the bowel again and again.
At the same time, this topic is easy to misunderstand. Some people hear “stem cells” and think miracle cure. Others assume it means aggressive transplant medicine with major risks. Neither simplification helps patients make clear decisions. Instead, the topic is more nuanced, and offers greater utility.
A New Hope for Managing Crohn's Disease
Consider a patient who has reached the point where every meal feels like a negotiation. They know where every restroom is. They don't commit to long drives. They read restaurant menus with more concern than enjoyment. Even on “good” days, Crohn's can sit in the background like a quiet threat.
That kind of daily vigilance changes people. It narrows life. It can also make every new treatment sound either too good to be true or too exhausting to pursue.
Stem cell therapy for Crohn's disease matters because it offers a different clinical idea. Instead of only trying to block one inflammatory pathway at a time, this approach aims to modulate the immune environment and support healing signals within damaged tissue. For patients who've already walked through standard care without durable relief, that shift can feel very meaningful.
A helpful way to think about it is this. Conventional therapy often works like lowering the volume on an alarm. Regenerative medicine asks whether the alarm system itself can be recalibrated.
That doesn't mean every patient is a candidate, and it doesn't mean every form of stem cell treatment is the same. It does mean there's a serious scientific and clinical reason this field has drawn attention, especially in inflammatory conditions. If you'd like a broader look at how cell-based approaches are used across immune-driven illness, this overview of stem cell therapy for autoimmune and inflammatory diseases gives useful context.
Crohn's care becomes more hopeful when the conversation shifts from “How do I suppress the next flare?” to “How do I help my immune system stop recreating the same pattern?”
For the right patient, that question can open the door to a new quality of life.
The Challenge of Conventional Crohn's Treatments
Crohn's disease is a chronic inflammatory disorder in which the immune system reacts in a way that damages the digestive tract. It can affect different areas, behave unpredictably, and change over time. That's one reason treatment can feel so uneven. What works for one patient may not work for another, and what worked last year may stop working this year.
Why standard treatment can feel like a ladder with missing rungs
Most patients move through care in stages. The exact sequence varies, but the pattern is familiar.
Anti-inflammatory medications may be used early, especially when clinicians are trying to calm active bowel inflammation.
Steroids can reduce inflammation more quickly, but they're generally not a good long-term strategy because of the burden they can place on the body.
Immunomodulators and biologics are designed to interrupt specific immune pathways and can be very important parts of modern Crohn's care.
Surgery enters the picture when complications such as strictures, fistulas, or severe damage become difficult to manage medically.
Each of these options can help. None should be dismissed casually. But many patients eventually discover the central limitation. Most conventional therapies are built to control disease activity, not to restore a healthier immune equilibrium in a durable way.
Common reasons patients start looking beyond standard care
Some patients respond well for years. Others don't.
A few patterns come up repeatedly in clinic conversations:
Loss of response over time. A medication that once worked stops holding the disease.
Incomplete control. Symptoms improve, but urgency, pain, fatigue, or dietary restriction remain.
Side effect burden. The treatment may help the bowel while creating new problems elsewhere.
Escalating complexity. More medications, more monitoring, more uncertainty.
Complications despite treatment. Fistulas, perianal disease, and repeated flares can continue even with advanced drugs.
Clinical reality: Many patients who ask about stem cells aren't rejecting standard medicine. They're looking for an option after standard medicine has left major gaps.
The underlying issue many patients sense
Patients often say, “It feels like my body is still stuck in attack mode.” That's a useful observation. Crohn's isn't only about visible inflammation on a scan or scope. It's also about the immune system continuing to receive, amplify, and repeat inflammatory signals.
Here's a simple comparison:
| Treatment focus | Main aim |
|---|---|
| Conventional drug therapy | Reduce or block parts of the inflammatory response |
| Regenerative cell therapy | Influence immune behavior and healing signals more broadly |
That doesn't make regenerative care a replacement for every standard therapy. It does explain why patients with persistent disease often become interested in a treatment model that tries to re-educate the inflammatory environment rather than only suppress it.
How Allogeneic Stem Cells Re-Educate the Immune System
A patient with Crohn's may hear “stem cell therapy” and picture damaged intestine being patched like torn fabric. That image misses the main mechanism. In Crohn's disease, the more relevant role of mesenchymal stem cells, or MSCs, is signaling.
MSCs work more like an air traffic control system than a construction crew. They do not need to become new bowel tissue to matter. They help coordinate how immune cells behave, how inflammation is contained, and how healing signals are released in injured tissue.
That distinction helps many patients make sense of why cell therapy can feel so different from the usual drug conversation.
How MSCs influence the immune environment
Crohn's disease involves an immune response that keeps reacting long after it should have settled. MSCs appear to affect that cycle by interacting with immune cells already active in the gut and surrounding tissues. The aim is not to erase immunity. The aim is to shift it away from constant alarm.
That is why many patients exploring advanced regenerative care spend time learning about immune modulation with stem cells. The phrase can sound technical. The practical meaning is simpler. The treatment is designed to calm misdirected inflammatory signaling while supporting a more organized healing response.
Why allogeneic cells matter
Allogeneic means the cells come from carefully screened donor tissue, not from the patient. That matters because it shapes both the biological strategy and the patient experience.
At Longevity Medical Institute, the treatment model described for Crohn's centers on a multi-tissue allogeneic approach, including placental, Wharton's jelly, adipose, endometrial, and dental pulp sources prepared through a biotechnology lab process. The clinical goal is immunomodulation and tissue support. It is a very different concept from the high-intensity autologous hematopoietic stem cell transplant protocols studied in some U.S. settings.
Patients often confuse these two categories because both are described loosely as “stem cell therapy.” They are not the same intervention. Autologous HSCT uses a patient's own blood-forming stem cells after an aggressive immune-conditioning phase intended to reset the immune system. The allogeneic MSC approach used here is designed around signaling, regulation, and recovery support through infusion-based care, without that same level of treatment intensity.
That difference is practical, not just scientific. It affects who may qualify, what the treatment days look like, and what level of risk a patient is being asked to accept.
What the cells appear to do
The clearest way to understand MSC activity is to separate it into three jobs.
Immune modulation. MSCs interact with T cells, B cells, macrophages, and other immune participants in ways that may reduce inflammatory signaling and encourage a more regulated response.
Paracrine signaling. They release bioactive factors that influence nearby cells. A useful comparison is a foreman sending instructions across a repair site rather than laying every brick personally.
Tissue support. They may improve the local conditions needed for mucosal healing, especially where inflammation has disrupted normal recovery.
Traditional medications often target one pathway at a time. MSC-based therapy appears broader in its signaling effects, more like changing the tone of the whole conversation inside inflamed tissue.
Why fistulas and perianal disease receive special attention
Perianal and fistulizing Crohn's disease highlight why this mechanism matters. These cases involve ongoing inflammation, poor tissue repair, and a local environment that struggles to close and remodel normally.
A meta-analysis reported on PubMed Central found that MSC therapy was associated with higher rates of perianal healing, fistula closure, and clinical remission compared with controls. Those findings fit the biology. A treatment that can influence both inflammatory signaling and wound-healing conditions is especially relevant in tissue that has been trapped in a cycle of breakdown and incomplete repair.
One point often reassures patients. The therapeutic effect does not appear to depend on the cells permanently living in the bowel. Research discussed earlier in the article suggests that the larger benefit may come from an early biologic message that changes how the immune system and local repair cells behave afterward.
For patients comparing options, this is the core idea to understand. The allogeneic MSC model used at LMI is not built around destroying and rebuilding the immune system. It is built around persuading an overreactive system to behave differently, while supporting healing in a setting designed to make the treatment process feel medically serious, carefully supervised, and logistically manageable for patients traveling to Los Cabos.
Reviewing the Clinical Evidence and Outcomes
A careful reading of the literature gives a more useful picture than hype or skepticism alone. The question is not whether stem cells have shown activity in Crohn's disease. They have. The more important questions are which type of cell therapy was studied, in which patients, and at what cost in risk.
One reason patients get confused is that very different treatments are often grouped under the same phrase, “stem cell therapy.” That is a little like putting a bone marrow transplant and a biologic infusion in the same bucket because both affect the immune system. They do not ask the body to do the same thing, and they do not carry the same burden.
What published outcomes actually show
Mount Sinai's review of stem cell transplants for Crohn's disease summarizes why the field remains interesting and cautious at the same time. In the studies they reviewed, many patients achieved remission in the months after treatment, but fewer maintained that result over longer follow-up. That pattern matters. Early response is encouraging. Long-term durability is still uneven.

For a patient, the practical takeaway is straightforward. Cell-based treatment may create a meaningful window of lower inflammation, better healing, and fewer flares. It does not promise a permanent reset for every person, and honest programs should say that clearly.
Why the type of transplant matters
The strongest published responses in severe refractory Crohn's have often come from autologous hematopoietic stem cell transplantation, or HSCT. In that model, physicians collect the patient's own blood-forming stem cells, suppress or ablate the immune system with intensive chemotherapy, and then reinfuse those cells. It is the closest thing in this field to rebooting a malfunctioning operating system by shutting the whole computer down first.
That intensity helps explain both the upside and the concern.
A CenterWatch listing for trial NCT04224558 shows how carefully this approach is still being studied in the United States. The trial is small, limited to patients who have failed conventional therapy, and specifically tracks transplant-related mortality and severe toxicity after HSCT. Those are not routine monitoring endpoints for a low-risk wellness intervention. They reflect the inherent hazards of immunoablation.
This distinction is one of the most important parts of informed consent. The high-risk autologous HSCT studied in US trials is not the same as the allogeneic, multi-tissue approach used at LMI. LMI's model is built around donor-derived cells selected for immune signaling and tissue-support effects, without first destroying the patient's marrow or forcing the body through chemotherapy-based immune wipeout. Patients comparing options deserve to see that contrast plainly.
A grounded way to read the evidence
The literature supports several reasonable conclusions:
| Question | What the evidence supports |
|---|---|
| Can cell therapy help selected patients with refractory Crohn's disease? | Yes. Published reports describe meaningful clinical responses in carefully chosen patients. |
| Are outcomes the same across all stem cell approaches? | No. Local MSC therapy, systemic allogeneic approaches, and autologous HSCT differ in mechanism, intensity, and risk. |
| Is fistulizing disease still one of the more promising targets? | Yes. The signal is especially interesting where inflammation and tissue repair problems overlap. |
| Does current evidence prove a permanent cure? | No. Response can be substantial, but durability varies and relapse remains possible. |
For many patients, that balanced framing is a relief. It replaces magical thinking with something more useful. A realistic chance of improvement, measured against real limits and real safety considerations.
Safety deserves the same attention as efficacy, especially for patients considering treatment outside their home country. A helpful companion resource is this review of stem cell safety and what our published research concluded.
Your Personalized Treatment Journey in Los Cabos
You may be sitting at home with a stack of colonoscopy reports, medication records, and lab results, wondering what treatment abroad would look like in real life. For many patients with Crohn's disease, that question matters as much as the science. Who reviews your case before you get on a plane? What happens when you arrive? How different is this from the high-risk transplant protocols you may have read about in U.S. trials?
A well-run program answers those questions in plain language, before any travel plans are made.
Before travel begins
The process usually starts with a remote physician review. Your records are examined closely, including diagnosis, prior medications, imaging, procedure reports, current symptoms, and complications such as strictures or fistulas. That early review helps sort out a central question. Is this a reasonable next step for your case, or would it be safer to delay, gather more information, or coordinate more closely with your gastroenterologist first?
That step is reassuring for patients who are considering care in Mexico and want more than a sales conversation. They want medical judgment.
Patients also tend to have practical concerns that are easy to underestimate until travel becomes real. Where will I stay? How far is the clinic from the airport? What does the treatment setting feel like? What kind of oversight is in place if I have questions during the week? A useful starting point is this overview of a stem cell clinic in Los Cabos and what patients should evaluate before treatment.
What happens on site
Once you arrive, the experience should feel organized, calm, and medically supervised. The model described by Longevity Medical Institute includes an in-person evaluation, in-house lab testing, and advanced imaging as needed to clarify the full picture before treatment decisions are finalized. Those operational details come from the clinic's described process, not from independent outcomes data, but they still matter because they shape safety and case selection.
The practical goal is straightforward. Confirm what kind of Crohn's disease you are dealing with, identify any factors that could change the plan, and match treatment to the patient in front of the team rather than to a generic protocol.
That often includes:
Case confirmation, including disease pattern, severity, prior treatment response, and current clinical priorities
Laboratory assessment, looking for inflammation, nutritional deficits, infection concerns, and other factors that may affect timing or safety
Targeted imaging or systems review when the history suggests a need for a broader picture
Individual treatment design, including cell source, route of administration, observation plans, and supportive care
The treatment philosophy is a key part of the patient experience. At LMI, the focus is on allogeneic cells from multiple tissue sources, used with the goal of immune modulation and tissue support. Patients often understand this best through a clinical analogy. An autologous HSCT strategy aims to erase and rebuild the immune system, which is a much more intensive process. An allogeneic MSC-based approach is closer to sending skilled mediators and repair crews into an inflamed environment so the system can calm down and heal more appropriately.
That difference changes the week on the ground in meaningful ways. The journey is built around evaluation, infusion-based care, observation, and follow-up planning. It is not structured like a chemotherapy-conditioned transplant admission.
To see the setting more concretely, this short video gives visual context for the patient experience:
Why patients compare this carefully
Patients exploring treatment abroad are usually comparing two things at once. They are comparing clinics, and they are comparing treatment models.
That distinction matters.
A luxury medical setting can make travel easier, but comfort alone is not the main issue. The primary clinical question is what kind of stem cell therapy is being offered. A lower-intensity allogeneic, multi-tissue approach is distinctly different from autologous HSCT protocols that involve immune ablation and a much heavier treatment burden. Patients deserve to see that difference clearly before they decide where to go.
Mexico-specific concerns also deserve direct answers. Serious patients want to know how records are handled, who is responsible for medical oversight, what monitoring is available during the stay, and how communication works once they return home. Those details often determine whether the experience feels secure or uncertain.
After treatment
Good follow-up is part of the therapy, not an afterthought. Patients need a clear plan for symptom tracking, hydration, nutrition, activity, medications, and communication with their local GI team. Early changes can be encouraging, confusing, or mixed, and each of those scenarios requires interpretation rather than guesswork.
Recovery is usually a monitored phase, not a single moment. The strongest programs treat it that way.
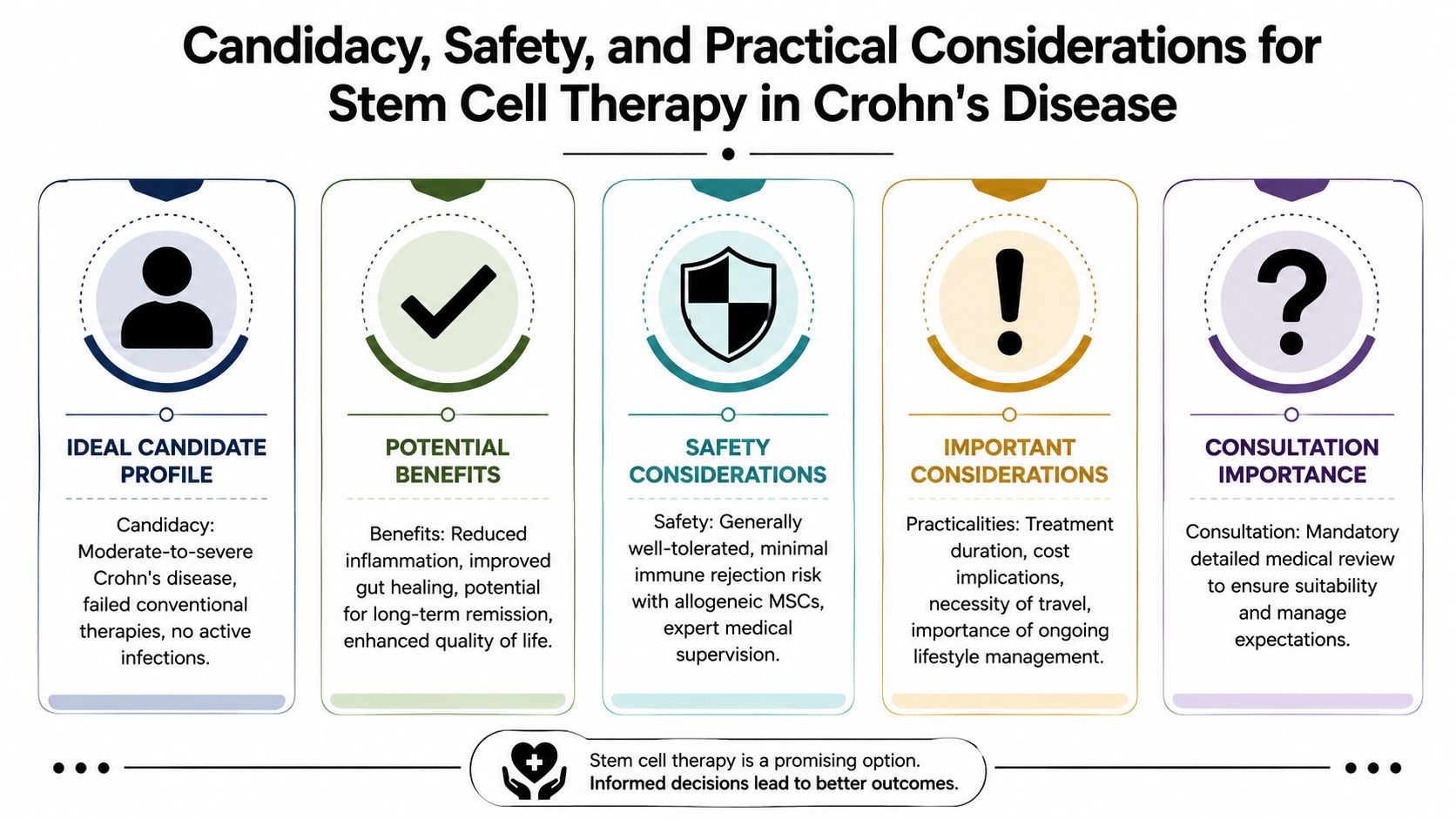
Candidacy Safety and Practical Considerations
A patient may look like a strong candidate on paper and still be a poor fit for treatment at a given moment.
Crohn's is not one disease experience. One person has inflammatory flares that keep breaking through medication. Another has fistulas, prior surgeries, weight loss, or a body that is too depleted to add another intervention safely. Good screening respects those differences. It asks not only, “Could stem cell therapy help?” but also, “Is this the right time, with this disease pattern, under these conditions?”
Who may be an appropriate candidate
Patients usually explore this option after the road has become complicated. That may mean moderate to severe disease, persistent inflammatory activity, incomplete response to standard therapy, medication intolerance, or challenging features such as fistulizing disease.
A careful evaluation usually looks at several layers at once:
How active is the disease right now? Active inflammation, structural damage, and fistula burden can point to different treatment goals.
What has already been tried, and how did the patient respond? Prior biologics, steroids, immunomodulators, and surgeries help define whether this is a reasonable next step.
Is there any active infection or medical instability? Infections, poor nutritional status, anemia, and recent complications may need attention first.
What result is the patient hoping for? Lower flare frequency, better daily function, less pain, and improved healing are reasonable goals. A guaranteed cure is not.
Why the treatment model matters so much for safety
Many patients hear the term “stem cell therapy” and assume all protocols carry the same level of risk. They do not.
The easiest way to understand the difference is to compare a system reset with a system calibration. Autologous HSCT, the high-intensity approach studied in severe refractory Crohn's, is built around immune ablation followed by reinfusion of the patient's own cells. That is a serious transplant-style process with a heavier risk profile, stricter candidacy standards, and a more demanding recovery.
The allogeneic, multi-tissue approach used at LMI follows a different clinical logic. It does not require wiping out the immune system first. The aim is to calm harmful immune signaling and support tissue repair using donor-derived cell populations selected for immunomodulatory and regenerative potential. For patients comparing options, that distinction is central. It changes the safety discussion, the travel burden, and the practical experience of treatment.
Lower intensity does not mean casual care. It means the questions are different. Instead of preparing for immune ablation, the focus is on screening for infection risk, medication interactions, current disease status, infusion tolerance, and short-term monitoring during the stay.
Practical questions about seeking care in Mexico
For a medical traveler, safety is partly clinical and partly operational. A well-run program should feel organized in the same way a good hospital service feels organized. Clear records. Clear responsibility. Clear follow-up.
That is especially important in Mexico, where patients from the US and Canada often arrive with understandable questions about regulation, oversight, emergency planning, and what their day-to-day stay will look like in Los Cabos. A luxury setting can reduce friction around travel, lodging, transportation, and recovery time. It does not replace medical discipline. The right program provides both.
Use questions like these to judge whether a clinic is prepared for serious Crohn's care:
| Question | Why it matters |
|---|---|
| Who is responsible for physician oversight of my case? | You need medical judgment, not only a coordinator answering logistics |
| Are the cells allogeneic or autologous, and what tissues are they sourced from? | The answer affects risk, intent, and how the treatment should be understood |
| How are records, consent, and treatment documentation handled? | Good documentation protects continuity of care after you return home |
| What screening could delay or disqualify treatment? | Ethical programs defer patients when timing or safety is not right |
| What monitoring is available during my stay in Los Cabos? | Patients should know who is watching for problems and how concerns are escalated |
| How will my home gastroenterologist be updated if needed? | Chronic disease care works better when local and travel-based care are coordinated |
For patients weighing these issues carefully, this guide on safety considerations for stem cell therapy in Mexico offers a useful starting framework.
A clinic should also be able to explain the patient journey in plain language. How many days you should plan to stay. What happens on evaluation day. How infusions are supervised. What support person, if any, should travel with you. Where concerns go after hours. Those details often tell you more about real safety than polished marketing does.
The human side of candidacy
Crohn's decisions are rarely only about biology.
Travel fatigue, missed work, childcare, nutrition during the trip, anxiety about being far from home, and coordination with a local GI team all shape whether treatment is realistic. Some patients are medically eligible but logistically overstretched. Others need a slower timeline so they can stabilize first. A thoughtful program says that openly.
The best consultation leaves a patient with clarity. They should understand whether they are a reasonable candidate, what risks need to be addressed, and what the trip to Los Cabos would ask of them. Pressure has no place in that conversation.
Beyond Symptom Management Real-World Results
A patient may arrive home after treatment and notice the first change in an ordinary moment. Breakfast feels less risky. A car ride no longer requires planning every stop. An evening out seems possible again.
That is often how meaningful progress appears in Crohn's disease. Subtly, in daily life.
Clinical discussions usually focus on inflammation, fistulas, bowel frequency, imaging, and medication use. Those measures matter. Patients live the disease in a different unit of measure. Can I eat without bracing for pain. Can I work through the afternoon. Can I sleep through the night. Can I say yes to travel, family plans, or exercise without worrying that my body will suddenly rebel.
For someone with fistulizing disease, improvement may mean less drainage, less tenderness, and the ability to sit comfortably. For someone with frequent flares, it may mean longer stretches of stability and fewer days lost to exhaustion. For another patient, the first win is a calmer relationship with food.
Recovery also tends to happen in layers, much like a room getting brighter as the sun comes up. You may not see everything change at once, but the pattern becomes clear over time. The first layer may be less inflammatory volatility. Then sleep improves. Then appetite feels safer. Then confidence returns.
Patients often describe progress in terms like these:
Longer periods between flares
Less disruption during work, meals, and travel
More comfort after eating
Less anxiety around social plans
A stronger sense of physical steadiness
As noted earlier, researchers are paying close attention to the possibility that mesenchymal signaling can leave behind a longer-lasting anti-inflammatory effect, even after the administered cells are no longer detectable. That idea helps explain why some patients report sustained improvement rather than a brief lift that fades quickly.
This distinction matters for patients comparing approaches. High-risk autologous HSCT, as studied in some U.S. settings, aims to reset the immune system through intensive conditioning and transplant-level medical risk. The allogeneic, multi-tissue model used at LMI is designed very differently. The goal is modulation, not ablation. In plain terms, it is closer to helping a misfiring orchestra return to tempo than stopping the entire performance and rebuilding the concert hall.
No responsible clinician should promise remission or a permanent response. Crohn's is too variable for that. The more honest goal is broader and, for many patients, more meaningful. Fewer inflammatory interruptions. Better function. More predictability. More room for life.
Sometimes the clearest sign of success is simple. The conversation stops revolving around symptom control and starts including plans, work, family, movement, and travel again.
The Longevity Medical Institute Advantage
The hardest part of evaluating stem cell therapy for Crohn's disease is separating precise care from vague marketing. Patients need specifics. What cells are used. How they're produced. Who reviews the case. How diagnostics shape the plan. What the treatment is trying to do biologically.
In that respect, the model described by Longevity Medical Institute is built around a defined allogeneic, multi-tissue approach rather than high-intensity transplant medicine. The author brief states that the institute's biotechnology lab produces five stem cell types, including placental, Wharton's jelly, adipose, endometrial, and dental pulp sources. It also describes an integrated care structure that combines regenerative therapy with advanced diagnostics and physician oversight.
That combination matters because Crohn's is rarely a one-variable disease. Patients don't just need a procedure. They need a plan that accounts for immune behavior, inflammatory load, nutritional status, structural complications, and long-term monitoring.
The broader lesson is simple. When you evaluate stem cell therapy for Crohn's disease, don't ask only whether a clinic offers cells. Ask whether the clinic can explain the treatment model with precision, align it with your medical history, and support you through the full decision process with clinical clarity.
For the right patient, that level of rigor can make regenerative medicine feel less mysterious and more like what it should be. A carefully designed medical option.
If you're exploring whether stem cell therapy for Crohn's disease may fit your case, Longevity Medical Institute offers physician-led consultations to review your history, discuss candidacy, and explain how allogeneic MSC-based care is structured in Los Cabos. A careful conversation is the right first step.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: May 20, 2026
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.