Stem Cell Therapy for Long COVID: A Patient's Guide
If you're reading this, there's a good chance life still hasn't returned to normal after COVID. You may be back at work, back to family routines, even back to exercise in a limited way, yet something still feels off. The fatigue doesn't match your effort. Your thinking feels slower than it used to. A short walk, a difficult meeting, or a poor night's sleep can leave you feeling as if your system has been pushed far beyond its limits.
For many people, that's the hardest part of long COVID. It can be severely disruptive while remaining largely invisible to everyone else.
As a clinician, I think it's important to start with reassurance and honesty. Your symptoms are real. They deserve a careful medical workup. And while stem cell therapy for long COVID has attracted serious interest, it should be approached with both hope and discipline. This is a developing area of regenerative medicine, not a shortcut and not a universal cure. The right conversation is not, "Can this fix everything?" The right conversation is, "In the right patient, under the right medical oversight, can this support recovery in a meaningful way?"
A New Hope for Healing from Long COVID
Long COVID often leaves patients stuck in a frustrating middle ground. Standard hospital tests may look acceptable, yet you still don't feel like yourself. You may have been told to wait, pace yourself, hydrate, sleep more, or give it time. Sometimes those steps help. Sometimes they don't help enough.
I often think of long COVID as a condition that can outlast the infection itself by leaving the body in a prolonged state of biological confusion. The virus may be gone, but the body may still behave as if it's responding to an ongoing threat. That can affect energy, cognition, breathing, circulation, sleep, exercise tolerance, and mood.
Why regenerative medicine enters the conversation
Regenerative medicine looks at a different level of the problem. Instead of focusing only on symptom suppression, it asks whether we can support repair, calm harmful inflammation, and help the body regain balance.
That doesn't mean stem cells are magic. It means they are being studied because they may act like biological coordinators. Rather than forcing a single pathway, they appear to send signals that influence how inflammation, immune activity, and tissue recovery unfold.
Long COVID can feel unpredictable to the patient because it may involve several systems at once. A treatment strategy has to respect that complexity.
For patients considering care across borders, especially from the United States or Canada, the attraction is understandable. You want thoughtful options. You want to know what is experimental, what is evidence-guided, what safety standards matter, and how to tell the difference between a real clinical program and a sales pitch.
Those are exactly the questions worth asking.
What Is Long COVID from a Cellular Perspective
Long COVID isn't just "feeling run down for longer than expected." At a cellular level, it appears to reflect a body that hasn't fully returned to its pre-infection baseline. The easiest way to understand it is to think of the body as an orchestra that lost its conductor during a crisis. The instruments are still there, but timing, rhythm, and coordination may remain off.
Chronic inflammation that doesn't fully shut off
Inflammation is a normal defense process. During acute infection, it helps the immune system respond quickly. The problem comes when that alarm system stays partly switched on after the immediate threat has passed.
In long COVID, many clinicians suspect that lingering inflammatory signaling may continue to affect tissues well after the acute illness. Patients often experience this not as "inflammation" in an abstract sense, but as exhaustion, body pain, post-exertional crashes, headaches, chest tightness, or a sense that recovery from small stresses takes far too long.
For a broader patient-friendly explanation of this process, our guide on stem cells for inflammation reduction explores how clinicians think about inflammatory load in chronic conditions.
Immune dysregulation and mixed signals
The immune system doesn't work like a simple on-off switch. It's more like a highly trained security team that must recognize danger, respond proportionately, and stand down when the threat has passed.
With long COVID, that handoff may not happen cleanly. Some patients appear to remain in a state of immune imbalance. In plain language, the system may keep sending mixed messages. One part is overreacting while another part isn't coordinating well. That can contribute to fluctuating symptoms and why some patients feel relatively normal one day and profoundly unwell the next.
Endothelial stress and tissue recovery problems
Another area of concern is the endothelium, the thin inner lining of blood vessels. You can think of it as the body's internal roadway surface. When that lining is irritated or damaged, circulation becomes less efficient. Tissues may receive oxygen and nutrients less smoothly, and the body's repair processes may slow down.
Long COVID often involves more than one organ system. A person may describe breathlessness, palpitations, brain fog, poor stamina, and muscle heaviness all at once. That pattern suggests the issue may not be isolated to one location. It may involve how tissues communicate, heal, and regulate blood flow.
Why patients get confused
Many people hear the term "cellular" and assume it means damage is permanent. That's not what it means. It means the problem may be happening at a finer level than routine exams can easily capture.
Clinical perspective: When symptoms persist after infection, the absence of a dramatic lab abnormality doesn't mean nothing is happening. It may mean the problem sits in regulation, signaling, and recovery.
That's why stem cell therapy for long COVID is even being discussed. The interest isn't based on hype alone. It's based on the idea that persistent symptoms may reflect a repair problem, not just a symptom problem.
Allogeneic Stem Cells: The Body's Master Repair Crew
When patients hear "stem cells," they often imagine cells that just turn into whatever the body needs. That picture is incomplete. In modern regenerative medicine, the cells most often discussed for inflammatory and post-viral conditions are mesenchymal stem cells, often shortened to MSCs. Their greatest value may come less from becoming new tissue and more from how they communicate with damaged or inflamed environments.
I often describe them as the body's master repair crew. Not because they do every job personally, but because they help organize the job site. They identify areas of stress, release signals that calm excess inflammation, and support the conditions needed for healing.
Why allogeneic cells are used
In our clinical model, we focus on allogeneic stem cells, meaning donor-derived cells rather than a patient's own cells. Patients are sometimes unfamiliar with that word, so it's worth making it simple. "Allogeneic" means the cells come from carefully selected donated tissue, not from your own body on the day of treatment.
Why does that matter? Because in regenerative medicine, cell quality matters. Patients with chronic illness, immune stress, or age-related decline may not have the most biologically optimal cells available for therapeutic use. Donor-derived cells from carefully prepared sources can offer a more standardized starting material.
At our center, the available cell sources include placental, Wharton's jelly, adipose, endometrial, and dental pulp lineages, all produced within an in-house biotechnology environment as part of physician-supervised regenerative programs. Patients who want a broader overview of this category can review our page on mesenchymal stem cell therapy.
What MSCs actually do
A useful analogy is to think of MSCs as expert project managers arriving at a building after a storm. They don't replace every broken beam themselves. Instead, they help coordinate cleanup, lower the chaos, and signal local crews to repair what can still be repaired.
That signaling role is why MSCs are being explored in conditions marked by inflammation, immune dysregulation, and tissue stress.
Some of the ways clinicians discuss their role include:
Inflammation support through signals that may help quiet an overactive environment
Immune balancing by influencing how immune cells behave
Repair support by encouraging a healthier healing response in stressed tissues
Vascular support through signals linked to blood vessel health and recovery
Exosomes as the message carriers
Patients also hear about exosomes, and the term can sound overly technical. An easy way to understand them is to think of them as sealed biological messages released by cells. These tiny packages carry instructions in the form of proteins, lipids, and other signaling contents.
If MSCs are the repair crew leaders, exosomes are the text messages and work orders they send out. They help relay what the surrounding tissue needs. In some protocols, clinicians are interested in exosomes because the therapeutic effect of MSCs may depend heavily on these signaling functions.
What this does and doesn't mean
This does not mean every stem cell product is the same. It doesn't mean every clinic handles sourcing, processing, or administration with the same rigor. And it doesn't mean cells can "find and cure" every symptom.
The most important question isn't whether a clinic says it offers stem cells. It's whether the clinic can clearly explain what type of cells it uses, why that cell type fits the condition, and how quality is controlled.
For long COVID, that distinction matters a great deal.
Targeting Long COVID: How Stem Cell Therapy Works
Long COVID can involve several overlapping problems at once. Ongoing inflammatory signaling. Immune confusion. Stressed blood vessels. Tissue recovery that never quite finishes. Stem cell therapy for long COVID is being explored because MSCs may address several of those layers at the same time.
Early in this conversation, it helps to see the logic visually.
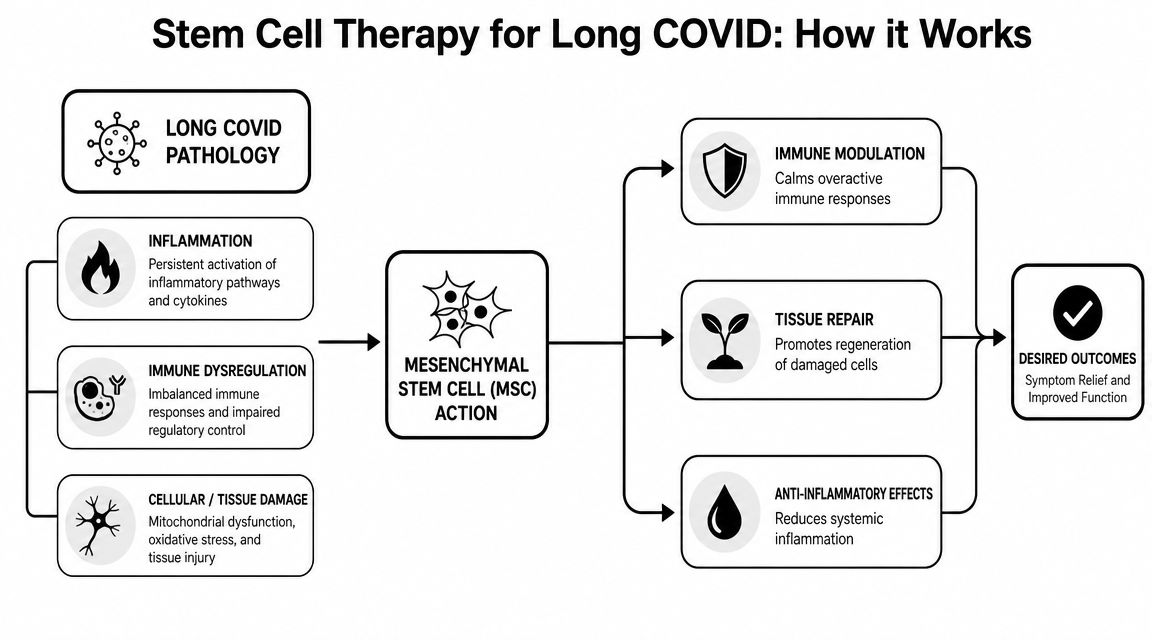
Calming an overreactive inflammatory environment
One of the main reasons MSCs attract interest in post-viral conditions is their potential anti-inflammatory effect. I don't mean anti-inflammatory in the same way as a pain reliever that temporarily suppresses symptoms. I mean something more nuanced. MSCs appear to send signals that may reduce the intensity of harmful inflammatory chatter within the body.
A helpful analogy is a room full of smoke detectors that continue blaring after a small kitchen fire has already been put out. The danger response made sense at first. But if the alarms keep sounding, normal life becomes impossible. MSCs are being studied as a way to help quiet that false emergency state. You can learn more by reading the research on Mesenchymal Stromal Cells as Modulators of Chronic Inflammation, Inflammaging, and Age-Related Disease: A Systematic Review.
Re-educating immune behavior
Long COVID may also involve immune dysregulation, where the immune system behaves less like a coordinated defense team and more like a group of responders receiving conflicting instructions.
MSCs are often described as immunomodulatory, not solely immune-suppressive. That's an important distinction. The goal isn't to shut the immune system down. The goal is to help it behave more appropriately.
For patients, this difference matters because many don't want to trade one problem for another. They're not looking to flatten all immune activity. They're looking for balance.
A more detailed explanation of these mechanisms appears in our overview of how stem cell therapy works.
Supporting vascular and tissue repair
Some long COVID symptoms suggest the body isn't delivering oxygen, nutrients, and recovery signals as efficiently as it should. If blood vessel lining and local tissues remain stressed, stamina drops. Recovery after exertion slows. Breathing may feel more effortful even when basic testing doesn't fully explain why.
MSC signaling is being studied for its potential role in supporting repair conditions around damaged tissues and blood vessels. The effect is similar to restoring communication and traffic flow after a storm has disrupted roads and utility lines. The cells don't rebuild an entire city overnight. They help create the conditions for organized repair.
Brain fog and neurological recovery
Brain fog is one of the most distressing long COVID symptoms because it touches identity itself. Patients say, "I don't feel sharp," or "I can't access my normal self." That experience may reflect neuroinflammation, autonomic disruption, poor sleep, circulation changes, or all of these together.
Researchers are interested in whether MSCs may help create a more favorable environment for neurological recovery by reducing inflammatory stress and improving system-wide regulation. That's not the same as promising restored memory or instant clarity. It means the therapy is being explored because cognitive symptoms may be tied to the same inflammatory and vascular biology affecting the rest of the body.
You can read more about the latest COVID-19 research here: Intravenous Mesenchymal Stromal Cells for Severe and Critical COVID-19: Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials
Why clinicians stay careful
All of this sounds promising because it is promising. But mechanism is not the same thing as proof of outcome. A therapy can make biological sense and still require careful study to determine when it helps, for whom it helps, and how much benefit is realistic.
That is why the best clinical conversations remain both optimistic and disciplined.
Current Clinical Evidence and Realistic Outcomes
Patients deserve a clear answer about the evidence. At this point, stem cell therapy for long COVID remains early and largely experimental.
A 2024 open-access review of stem cell therapy in COVID-19 and related conditions noted that more than 100 clinical trials registered on ClinicalTrials.gov were exploring mesenchymal stem cells or MSC derivatives in COVID-19, but most endpoints were safety-focused and efficacy findings were often inconclusive, especially in mild-to-moderate disease. The same review also emphasized that while some studies in severe or critically ill patients showed improvement in oxygenation, lung function, or inflammatory markers, the overall evidence was still insufficient to establish MSC therapy as a standard treatment for post-COVID conditions.
That distinction matters. Much of the earlier work was not designed around the patient sitting at home months later with fatigue, brain fog, and post-exertional setbacks. It was built around acute COVID, severe illness, and immediate safety questions.
Why the newer long COVID trial matters
A meaningful shift appears in a randomized, double-blind, placebo-controlled ClinicalTrials.gov study for WHO-defined long COVID. This study, listed as NCT06492798, plans to enroll 76 participants. Its first safety stage includes 10 patients all receiving umbilical cord mesenchymal stem cells (WJ-MSC's). A second stage includes 66 participants randomized 1:1 to treatment versus placebo, with outcomes tracked at 28 days, 12 weeks, and 24 weeks using CTCAE 5.0 symptom scores.
For patients, this is important not because it proves success in advance, but because it shows the field is moving toward more rigorous long-COVID-specific testing. That's a different scientific question from asking whether MSCs were tolerated during acute respiratory failure.
What realistic outcomes look like
In real clinical decision-making, the honest expectation is not "cure." It's possible improvement in function, symptom burden, and recovery capacity, with meaningful variation from patient to patient.
Some patients may care most about fatigue. Others are driven by brain fog, shortness of breath, dysautonomia-like symptoms, or a general inability to return to exercise and work. Because long COVID isn't a single uniform disease pattern, response is unlikely to look identical across all patients.
A practical way to think about expectations is this:
| Focus area | Realistic framing |
|---|---|
| Symptom relief | Possible, but not guaranteed and rarely immediate |
| Functional improvement | Often more clinically meaningful than chasing perfect symptom elimination |
| Timeline | Recovery may unfold gradually rather than all at once |
| Best use case | Often as part of a broader physician-guided plan, not a stand-alone miracle intervention |
Evidence note: The science is evolving in the right direction, but it hasn't reached the point where any responsible clinician should present stem cells as established standard care for long COVID.
Patients exploring treatment should also understand that good medicine starts with diagnosis. Long COVID can overlap with autoimmune activity, endothelial dysfunction, persistent inflammation, sleep disruption, mast cell patterns, cardiopulmonary issues, and autonomic disturbance. That's one reason broader resources on stem cell therapy for autoimmune and inflammatory diseases can be useful when thinking through the inflammatory side of the picture.
The Longevity Medical Institute Care Pathway
For a patient traveling from the United States or Canada to Mexico, the most important question usually isn't just "Do you offer stem cells?" It's "How do you decide whether stem cells are appropriate for me, and what surrounds the treatment?"
That's where the care pathway matters.
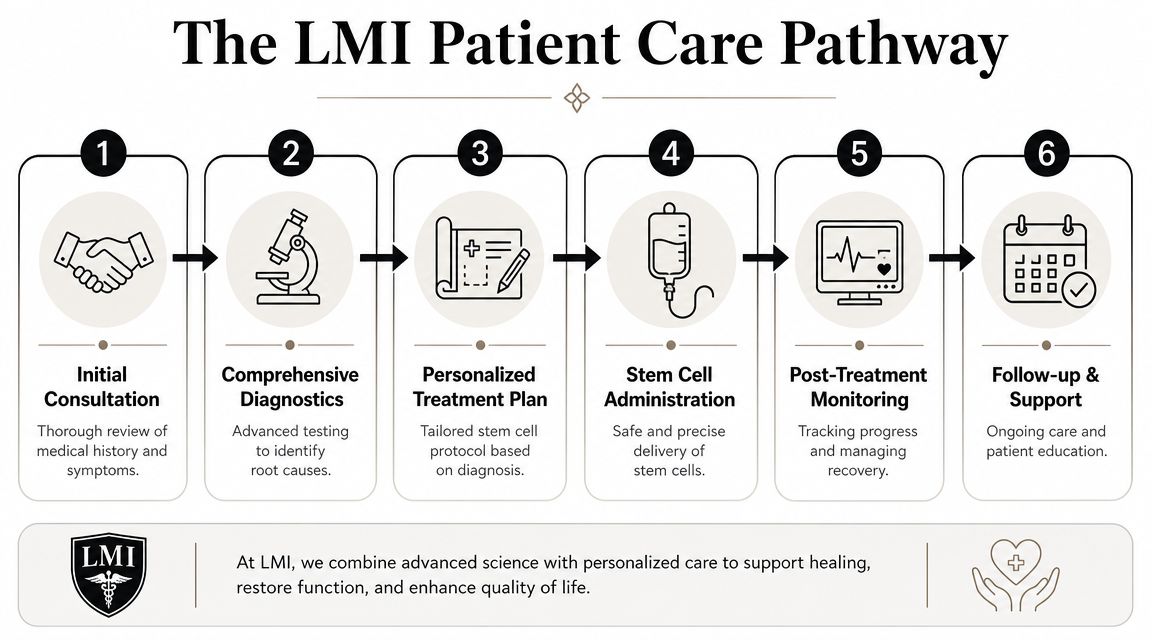
The evaluation comes first
At Longevity Medical Institute, stem cell therapy sits inside a physician-led workup rather than replacing one. A patient with long COVID may arrive focused on fatigue, but the clinical team still needs to ask harder questions. Is there cardiopulmonary strain? Autonomic dysfunction? Ongoing inflammatory burden? Sleep pathology? Nutrient depletion? A silent recovery barrier that hasn't yet been identified?
That workup may include an in-house clinical laboratory measuring a broad biomarker panel, advanced heart evaluation, and AI-integrated full-body MRI when clinically appropriate. Those tools don't diagnose long COVID by themselves. They help clinicians understand the terrain the therapy would be entering.
Building a personalized protocol
No serious regenerative program should treat long COVID as a one-size-fits-all package. Two patients can share the same label and have very different dominant patterns.
One patient may have exertional crashes and inflammatory symptoms. Another may have brain fog, poor sleep, and autonomic instability. Another may still show lingering respiratory vulnerability. The treatment plan has to reflect that.
That personalized plan may include:
Cell selection based on the physician's assessment and the biologic goals of care
Route of administration such as intravenous delivery when systemic support is the clinical focus
Supportive therapies chosen to reduce physiologic friction around recovery
Monitoring strategy so the patient's response is tracked rather than guessed at
What treatment day often feels like
Patients are often anxious about the procedure itself. In a properly run program, treatment shouldn't feel chaotic or improvised. It should feel medical, calm, and structured.
Intravenous administration is commonly discussed for systemic conditions because the therapeutic goal isn't a single injured joint. The aim is broader signaling support across inflammatory, vascular, and immune pathways. The clinical team reviews indications, checks readiness, administers treatment in a monitored setting, and observes the patient appropriately afterward.
Good regenerative care feels less like buying a product and more like entering a monitored treatment relationship.
Why adjunctive therapies may matter
Long COVID rarely involves one isolated mechanism, so many programs pair stem cell therapy with supportive care. Depending on the patient's needs, that may include hyperbaric oxygen therapy, peptide-based protocols, targeted IV support, sleep-focused evaluation, physical medicine strategies, or cardiometabolic follow-up.
The goal isn't to pile on interventions for the sake of complexity. The goal is to reduce obstacles that can blunt recovery. If tissues are under-oxygenated, sleep is fragmented, and inflammation remains high, even a thoughtful regenerative intervention may not perform as well as it could in a better-supported physiologic environment.
Follow-up is part of the treatment
One of the biggest misunderstandings in medical tourism is the belief that the treatment is the infusion and everything else is optional. That approach is too thin for a condition as layered as long COVID.
Patients need a clear follow-up plan. That includes symptom tracking, physician communication, and a framework for what to do if progress is slower than hoped or if another issue becomes more visible as recovery begins. The best care pathway doesn't stop when the patient leaves the clinic. It accounts for what happens after.
A Patient's Guide to Choosing a Clinic in Mexico
Mexico has become an important destination for patients seeking regenerative care, but quality varies. If you're considering stem cell therapy for long COVID, your job isn't to find the clinic with the boldest promises. Your job is to find the clinic with the clearest answers.
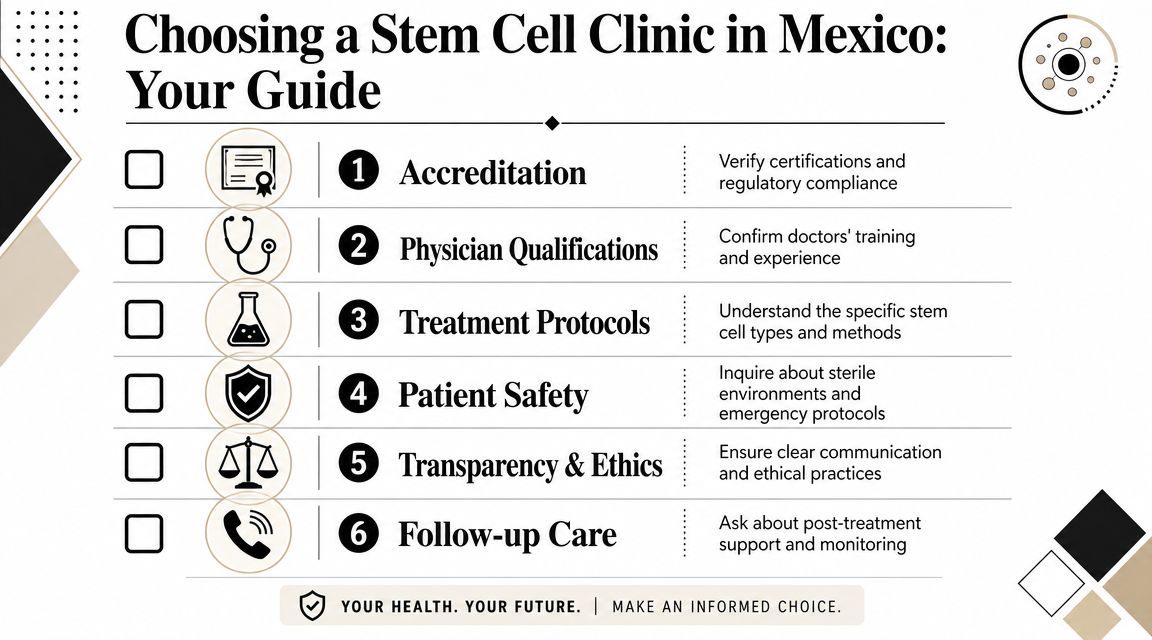
Questions that separate real medicine from marketing
A reputable clinic should be able to answer practical questions without evasion.
Ask about the following:
Cell source and type
What cells are being used? Are they allogeneic MSCs? From what tissue source? Why does the clinic believe that source fits long COVID?Laboratory control
Does the clinic rely on an in-house biotechnology lab or third-party procurement? How does it handle sterility, documentation, and quality control?Medical leadership
Who evaluates you medically? Who reviews your records? Who administers treatment? Are licensed physicians directly involved?Regulatory standing
Is the clinic operating within applicable Mexican regulatory requirements, including COFEPRIS-related oversight where relevant?Emergency readiness
If a patient has a reaction, what happens next? Is there a protocol, trained staff, monitoring equipment, and escalation capacity?Follow-up plan
What support exists after treatment, especially once you return home to the U.S. or Canada?
For readers comparing options, our clinic selection guide on choosing a stem cell clinic in Mexico gives a broader checklist.
Red flags to take seriously
Some warning signs are simple. If a clinic guarantees results, avoids discussing limitations, or treats your questions like obstacles to the sale, step back.
A few red flags to watch for:
| Red flag | Why it matters |
|---|---|
| Guaranteed outcomes | Long COVID is too complex for honest guarantees |
| Vague cell descriptions | If they can't name the product clearly, you can't assess the treatment clearly |
| No real medical workup | Therapy without diagnosis is guesswork |
| Pressure to book immediately | Good clinics don't need urgency tactics |
| Thin aftercare | Follow-up is part of safety, not an optional extra |
If a clinic makes stem cells sound simple, the clinic may not understand the condition well enough.
A practical standard for medical tourists
For U.S. and Canadian patients, travel adds another layer. You're not only evaluating the procedure. You're evaluating the entire episode of care. That includes pre-travel review, airport-to-clinic logistics, treatment-day monitoring, communication with your home physicians when needed, and realistic instructions for the recovery period.
The right clinic should be able to explain the process in plain language. Not with hype. With specifics.
Long COVID often leaves patients vulnerable to overselling because they've already tried many things and are exhausted. That makes discernment even more important. A well-designed program won't promise certainty. It will offer a careful diagnostic process, a biologically coherent rationale, and a safety framework strong enough to deserve your trust.
Article Information and Disclaimer
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: May 24, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.
If you'd like a physician-led review of whether stem cell therapy for long COVID fits your situation, you can contact Longevity Medical Institute. A proper next step is a consultation that reviews your symptoms, prior testing, travel considerations, and whether a broader diagnostic and regenerative plan makes medical sense for you.