Stem Cells for Ligament and Tendon Repair: A Patient Guide
A tendon or ligament injury can change your life in quiet, frustrating ways. You stop trusting your shoulder overhead, your knee on stairs, or your ankle on uneven ground. You rest, ice, modify training, try physical therapy, and maybe even get temporary relief, yet the tissue never seems to return to its old strength.
That pattern is common because these injuries often become chronic long before they become dramatic. The pain may ease, but the tissue quality doesn't always recover well. For active adults, golfers, tennis players, runners, and patients who want to move without hesitation, that gap matters.
Stem cells for ligament and tendon repair are often discussed in broad, confusing terms. Patients hear promises, but they don't always get a clear explanation of what the therapy is trying to do, who it may help, and what a careful treatment pathway should look like. A sound clinical decision starts with understanding the biology, the evidence, and the quality controls behind the treatment.
A New Approach to Healing Stubborn Injuries
If you've been dealing with a stubborn tendon or ligament injury, you've probably already done many of the "right" things. You may have reduced activity, completed rehab, changed shoes, used braces, or adjusted your workouts. Sometimes those steps help. Sometimes they only keep the problem from getting worse.
The reason regenerative medicine draws so much attention is simple. It doesn't focus only on suppressing symptoms. It aims to support the actual repair environment inside damaged tissue. That matters in structures like the rotator cuff, Achilles tendon, patellar tendon, plantar fascia, or partial ligament injuries, where healing often stalls.
A useful way to think about this is the difference between pain control and tissue restoration. Pain control may reduce inflammation or limit movement. Tissue restoration tries to improve how the injured area organizes and rebuilds itself over time.
Clinical perspective: The key question isn't only "How do we calm this down?" It's also "How do we improve the quality of healing?"
The discussion now turns to stem cells for ligament and tendon repair. In modern orthopedic regenerative medicine, the focus is on how these cells influence the healing environment, support collagen remodeling, and help shift an injury away from chronic irritation and toward organized repair.
For readers who want a broader foundation in regenerative care, cell regeneration therapy provides useful background on how these therapies are positioned in clinical practice.
What makes this approach different
Traditional care often works from the outside in. Rest changes load. Physical therapy changes mechanics. Anti-inflammatory strategies change symptoms. Those tools can be valuable, but they don't always solve the biological bottleneck inside poorly healing tissue.
Regenerative care works from the inside out. The goal is to improve the signaling environment at the injury site so the tissue has a better chance to remodel in a more functional way.
That doesn't mean every injury needs stem cell treatment. It means some chronic injuries need more than patience.
Why Ligaments and Tendons Heal So Slowly
A common clinical scenario looks like this. A patient sprains an ankle, strains a hamstring tendon, or develops chronic elbow pain. The first few weeks seem manageable. Then progress slows, activity resumes, and the same tissue becomes irritated again. That pattern is frustrating, but it is not random. Ligaments and tendons are among the slower tissues in the body to repair well.
Their job explains part of the problem. Tendons transfer force from muscle to bone. Ligaments stabilize joints and control motion. To do that, they are built from dense, highly organized collagen fibers designed for tension and durability. That structure is excellent for load-bearing, but it is less favorable for fast biological repair.
Blood flow is the other major issue. Compared with tissues that heal more readily, many tendons and ligaments have a more limited vascular network. After injury, fewer blood vessels means slower delivery of oxygen, nutrients, signaling molecules, and repair cells. Recovery can still happen, but the margin for efficient healing is smaller.
A practical comparison helps here. A well-perfused tissue functions like an area with multiple supply routes and rapid maintenance access. Tendon and ligament tissue often functions more like a site reached by a narrower road with fewer support crews. If demand rises after injury, the repair process can lag behind.
Why some injuries stop improving
In the early phase, the body usually mounts a repair response. The problem is quality control. Instead of rebuilding tissue with the same alignment and mechanical integrity it had before, the body may produce a patch that closes the gap but does not fully restore performance.
That is why patients can feel "better" without being fully healed.
Several biological patterns drive that stalled recovery:
Disorganized collagen: Strong tendons and ligaments depend on collagen fibers lining up in a precise direction. Injured tissue often heals with a less orderly pattern.
Prolonged irritation: Inflammation should help initiate repair, then settle. In chronic injuries, that transition may be incomplete.
Scar-heavy healing: Scar tissue can add short-term stability, but it usually tolerates load less effectively than well-remodeled native tissue.
Repeated mechanical stress: Walking, gripping, lifting, and sports all keep loading the tissue while it is trying to recover.
For patients working through early or moderate overuse problems, our guide on how to heal tendonitis faster with conservative strategies explains where rest, load modification, and rehabilitation still fit.
Why premium regenerative care starts with better diagnosis
Another reason these injuries linger is that the label can be too simple. "Tendonitis" may involve degeneration, partial tearing, failed collagen remodeling, joint instability, or compensation from a nearby structure. "Ligament injury" may include subtle laxity that standard imaging misses.
That is why an integrated pathway matters. At a center such as Longevity Medical Institute, the process does not start with cells. It starts with defining the problem accurately through specialist assessment, functional examination, and advanced imaging, including AI-supported MRI interpretation when appropriate. If the biology is stalled, treatment planning can then match the tissue state, tear pattern, load demands, and recovery goals.
Why standard treatment can plateau
Rest can reduce strain. Physical therapy can improve mechanics and load tolerance. Injections may help with pain in selected cases. Surgery can repair certain tears or restore stability when structure is clearly compromised.
Each of those tools has a role. The limitation is that slow-healing connective tissue often needs more than symptom control or mechanical protection. It may need a better local healing environment, careful cell selection, and a recovery plan that supports remodeling after treatment. In high-standard regenerative medicine, that means a coordinated pathway from diagnosis to lab processing to post-procedure rehabilitation, rather than a one-step intervention.
Poor blood supply does not prevent healing. It makes healing slower, less organized, and more likely to produce tissue that is serviceable but not fully resilient.
How Allogeneic Stem Cells Guide Regeneration
The most important concept to understand is this. Mesenchymal stem cells, often called MSCs, are not just replacement parts. In orthopedic care, their main value is that they act like intelligent biological coordinators.
Rather than functioning only by becoming new tendon or ligament tissue, MSCs help organize the environment around an injury. They send signals that influence inflammation, blood vessel formation, cellular activity, and matrix remodeling. In plain language, they help the body shift from a stalled repair pattern to a more constructive one.
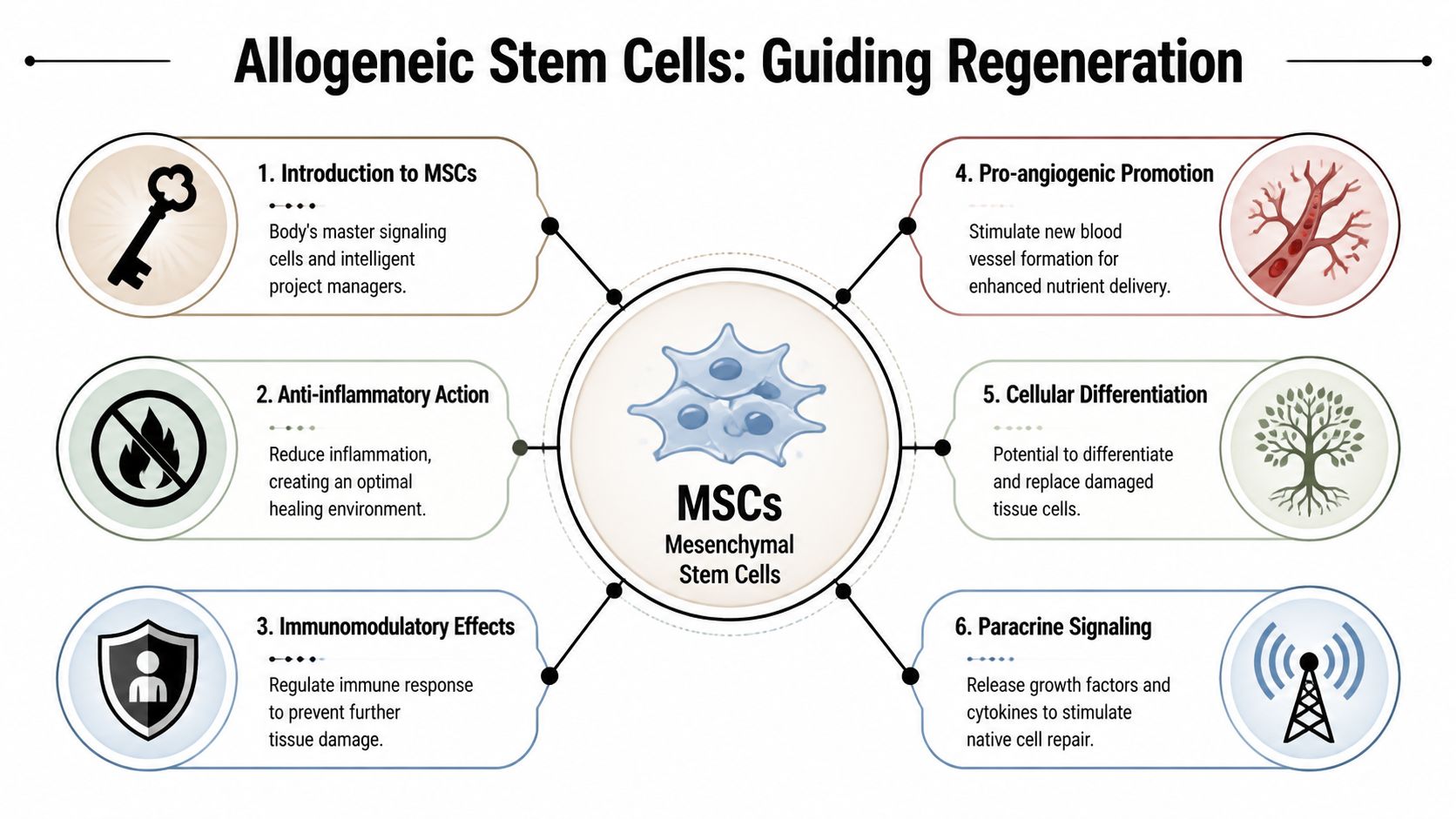
A detailed review on MSC-based tendon repair describes four core mechanisms. MSCs help by reducing inflammation, promoting neovascularization, enhancing cell proliferation and differentiation, and reorganizing extracellular matrix, with clinical doses typically requiring over 10 million cells (10^6–10^7) for substantive regeneration (PMC review on MSC mechanisms in tendon repair).
The project manager model
When patients hear "stem cells," they often picture the cells turning directly into brand-new tissue. That can happen in limited ways, but it isn't the best frame for understanding treatment. A better frame is the project manager model.
A project manager doesn't build the entire structure alone. The manager coordinates teams, timing, communication, and quality. MSCs do something similar biologically.
They can help:
Calm the environment so excessive inflammation doesn't keep damaging tissue
Recruit native repair responses already present in the body
Encourage new microvascular support so the area receives better biological input
Guide collagen remodeling toward a stronger, more functional structure
This is one reason stem cells for ligament and tendon repair have become so important in regenerative orthopedics. The therapy isn't just trying to patch tissue. It's trying to improve how tissue heals.
Why allogeneic matters in our model
In our clinical model, we use allogeneic cells only. That means the cells are sourced from carefully screened donor tissue rather than taken from the patient at the time of treatment. We don't use autologous stem cells.
That distinction matters because the treatment philosophy is different. The focus is on high-quality, lab-produced cell preparations from specific allogeneic sources. Our biotechnology lab produces five types of stem cells, including placental, Wharton's jelly, adipose, endometrial, and dental pulp cell lines.
For patients researching mesenchymal stem cell therapy, this is an important point of clarity. The source, handling, quality control, and delivery strategy all influence the clinical rationale for treatment.
Why cell source and delivery both matter
Not every tendon or ligament problem is identical. Some injuries involve a degenerative tendon. Others involve a partial ligament tear, a poor-quality surgical bed, or a chronic insertional problem. A careful clinician thinks not only about whether stem cells are appropriate, but also about the likely tissue behavior and how best to deliver them.
This is why high-level programs don't reduce care to "an injection." They build treatment around diagnosis, image guidance, biologic selection, and recovery planning.
The procedure is brief. The biology is not. Most of the real work happens in the quality of planning before the injection and the quality of tissue remodeling after it.
The Clinical Evidence for Tendon and Ligament Repair
A reasonable patient should ask a simple question. Has this approach held up in real tissue over real time, or does it only look promising in the first few months?
One of the clearest clinical signals comes from rotator cuff repair, where cell-based augmentation has been associated with better long-term structural integrity than standard repair alone. That matters because pain scores can improve for many reasons, but an intact repair years later points to something deeper. It suggests the healing environment changed in a meaningful way.
At 10-year follow-up, the MSC-augmented group in that landmark rotator cuff study showed substantially higher rates of intact repair than the control group, as noted earlier in the article. For a patient, the practical meaning is straightforward. The goal is not only early symptom relief. The goal is a repair that remains sound after the tissue has been tested by everyday life.
What patients should take from that evidence
Rotator cuff data is useful because the shoulder gives us a demanding real-world model. Tendon tissue has to reattach, organize collagen, tolerate load, and keep performing long after formal rehabilitation ends. If a biologic strategy helps in that setting, it strengthens the rationale for selected tendon and ligament injuries elsewhere in the body.
That does not mean every tendon problem should be treated the same way.
A partial tear, a degenerative tendon, and a fully retracted injury are different problems. A high-standard clinic interprets evidence through the lens of diagnosis, tissue quality, biomechanics, and imaging. At Longevity Medical Institute, that is why the evidence review sits inside a broader pathway that includes advanced assessment, image-guided delivery, controlled cell sourcing, and structured recovery support rather than a one-size-fits-all injection model.
If your concern is the shoulder specifically, our page on stem cell therapy for rotator cuff tear explains that application in more detail.
Evidence beyond the shoulder
The broader literature in tendon and ligament healing points in the same biological direction. Across preclinical and early clinical settings, investigators have observed better collagen organization, more orderly tissue architecture, and improved healing behavior when the right cells are used in the right environment. A useful analogy is scaffolding at a construction site. The cells do not only fill a gap. They help coordinate the repair crew, support the local environment, and encourage the tissue to rebuild in a more organized pattern.
That distinction matters for chronic injuries. A painful tendon often is not just inflamed. It may be disorganized, poorly vascularized, and mechanically unreliable. In those cases, the quality of the clinical pathway matters as much as the product itself. Better diagnostics help identify the actual pain generator. Better lab controls help define what is being delivered. Better recovery planning, including tools such as HBOT when appropriate, supports remodeling after the procedure.
A short visual overview can help if you're trying to connect the science to real orthopedic anatomy.
Why evidence still needs clinical judgment
Published data can support a treatment category, but it cannot choose the right patient. That decision comes from matching the biology to the injury pattern.
A patient with chronic tendinopathy and poor tissue quality may be a reasonable regenerative candidate. A patient with a fully retracted tear, gross instability, or a structure that needs mechanical reconstruction may need surgery first, or surgery plus biologic support. Good clinical care separates those groups carefully. The evidence is strongest when it is applied inside a quality-controlled system, from diagnosis through recovery, with clear expectations about what biologic treatment can and cannot do.
Comparing Stem Cells to Surgery and PRP
Patients usually aren't deciding in a vacuum. They're choosing between ongoing conservative care, PRP, surgery, or stem cell-based treatment. Each option has a role. The key question is which one matches the tissue problem and the patient's goals.
Surgery can be necessary when structure must be mechanically restored. PRP can be useful when a patient needs a simpler orthobiologic signal. Stem cells sit in a different category because they offer broader biological orchestration of healing.
Treatment Option Comparison Ligament and Tendon Injuries
| Feature | Stem Cell Therapy | PRP (Platelet-Rich Plasma) | Surgery |
|---|---|---|---|
| Primary goal | Support regenerative signaling and tissue remodeling | Deliver concentrated growth factors from platelets | Mechanically repair or reconstruct damaged tissue |
| Invasiveness | Minimally invasive injection-based procedure | Minimally invasive injection-based procedure | Operative procedure with incisions and tissue disruption |
| Biological role | Broader signaling effects on inflammation, vascular support, cell activity, and matrix organization | Growth factor support, often used as a biologic booster | Structural correction rather than biologic orchestration |
| Recovery pattern | Usually gradual remodeling over time | Usually gradual, often used in less severe cases | Recovery depends on procedure and rehab demands |
| Best fit | Chronic tendinopathy, partial tears, selected ligament or tendon injuries | Milder tendon issues or adjunctive care | Major tears, retraction, instability, or failed conservative care |
| Limitation | Requires precise diagnosis, quality-controlled product, and expert delivery | May not provide the same depth of regenerative signaling | More invasive, with surgical risk and longer rehabilitation |
The PRP distinction
PRP can be helpful, and many patients benefit from it. But PRP is not the same as stem cell therapy. Platelets release growth factors. MSCs influence a wider healing network.
That distinction becomes important in more stubborn injuries where tissue remodeling quality matters more than a short-term stimulus.
The surgery distinction
Surgery addresses structure. That's sometimes exactly what's needed. If a tendon is fully ruptured or a ligament injury has created clear instability, surgery may be the most appropriate option.
But surgery doesn't automatically produce ideal biology. It creates a repair, then depends on the body to heal around that repair. In selected patients, regenerative therapies may be considered as part of a strategy to support tissue quality.
A newer branch of the science also points to the importance of cell type selection. Research on tendon-derived stem cells suggests they have superior tenogenic potential over more general bone marrow stem cells, with up to 85% restoration of biomechanical strength in animal models (Frontiers review on tendon-derived stem cells and tendon healing). For patients, the takeaway is straightforward. Precision matters. The right biologic tool should match the tissue problem.
Your Treatment Pathway at Longevity Medical Institute
The quality of a stem cell procedure depends on much more than the injection itself. A premium clinical pathway starts with diagnosis, moves through biologic selection and guided delivery, and continues into recovery support. Patients often focus on the product, but the process is just as important.
Step one is mapping the injury correctly
A careful workup should answer several questions. Is the pain coming from the tendon or ligament? Is the problem degenerative, partially torn, surgically altered, or compensatory? Is there joint instability, nerve contribution, or adjacent tissue overload?
In a more integrated setting, that assessment may include:
Diagnostic ultrasound for real-time evaluation of tendon structure and focal defects
MRI review, sometimes as part of broader imaging workups, to assess tissue quality and associated pathology
Functional exam to identify loading errors, instability patterns, or kinetic chain contributors
Advanced diagnostics when the case is more complex and symptoms suggest broader contributors to recovery capacity
For medical travelers and complex orthopedic cases, some clinics also integrate AI-supported full-body MRI and broader health assessments to identify hidden factors that may affect healing readiness.
Step two is selecting the biologic strategy
On this point, many online discussions become too simplistic. A proper program doesn't treat every tendon and ligament issue with the same formula. It considers injury location, chronicity, tissue quality, prior procedures, and the broader recovery environment.
Longevity Medical Institute is one option patients evaluate when they want a physician-led pathway that combines advanced diagnostics, a COFEPRIS-licensed biotechnology lab, image-guided regenerative procedures, and recovery support under one roof.
In our practice model, that biologic pathway is based on allogeneic cell therapy only. The lab produces five stem cell types: placental, Wharton's jelly, adipose, endometrial, and dental pulp. The practical reason for this approach is consistency, controlled processing, and treatment planning built around high-standard laboratory production rather than same-day patient tissue harvest.
Step three is precise delivery
For ligament and tendon injuries, image guidance matters. A biologic treatment should be placed where the pathology is, not where it is assumed to be. Ultrasound-guided procedures allow the clinician to visualize the tendon fibers, insertion site, sheath, or ligament target and place the injectate with far greater precision than an unguided approach.
That matters in structures such as:
Rotator cuff tendons
Patellar tendon
Achilles tendon
Plantar fascia
Medial or lateral elbow tendons
Selected ligament injuries around the knee or ankle
Step four is supporting the recovery window
A stem cell treatment isn't finished when the patient leaves the procedure room. Tissue remodeling happens over time, and that period needs structure.
Depending on the case, supportive care may include:
Physical medicine and rehabilitation to guide safe reloading
Hyperbaric oxygen therapy to support recovery conditions
Follow-up imaging when clinically indicated
Activity progression planning so patients don't overload tissue too early
Practical rule: The injection creates an opportunity. The recovery plan determines whether the tissue gets the right mechanical signals afterward.
For international patients, logistics matter too. A smooth pathway includes coordination of consultation, diagnostics, treatment scheduling, and follow-up guidance so the experience feels organized rather than fragmented.
Safety Patient Selection and Expected Results
Patients should be skeptical of any program that talks only about benefits. Stem cells for ligament and tendon repair can be promising, but they are not casual wellness add-ons. They are medical treatments that require diagnosis, patient selection, and disciplined product quality.
One under-discussed issue is aberrant healing. As noted in a review discussing tendon-derived stem cells, stem cell responses can sometimes contribute to scar tissue formation rather than ideal regeneration if they are not precisely modulated and delivered. That is exactly why product quality, targeting, and clinical judgment matter so much.
Who may be a reasonable candidate
In general, the better candidates are patients with:
Chronic tendinopathy that hasn't responded adequately to conservative care
Partial tears where tissue quality still gives regeneration a realistic role
Persistent pain with imaging correlation rather than vague, unexplained symptoms
A willingness to follow a staged recovery plan instead of expecting an overnight fix
A patient may be less suitable if the tissue is too structurally compromised, if instability clearly requires surgery, or if the diagnosis itself is uncertain.
For a broader discussion of risk frameworks and clinic standards, is stem cell therapy safe is a useful reference, as well as this study Safety of Allogeneic Mesenchymal Stromal Cell Therapy Across Human Clinical Indications: A Systematic Review of Landmark Clinical Trials and Published Safety.
What results usually feel like
The timeline is usually gradual. These therapies don't work like a local anesthetic. The goal is not a dramatic same-day transformation. It's progressive tissue remodeling and a better healing trajectory.
Patients often notice the process in phases:
Early period: Some soreness or post-procedure awareness is common.
Intermediate phase: Day-to-day irritation may begin to settle, though loading tolerance is still limited.
Remodeling phase: Strength, confidence, and function improve as rehab progresses.
What reduces risk
High-level safety isn't one thing. It's a chain of decisions.
Screened donor sourcing
Controlled lab processing
Sterile handling
Accurate diagnosis
Image-guided delivery
Recovery oversight
When those pieces are weak, results become less predictable. When those pieces are strong, treatment is more likely to support organized healing rather than a poorly directed response.
Frequently Asked Questions
| Question | Answer |
|---|---|
| Are stem cells for ligament and tendon repair the same as PRP? | No. PRP mainly delivers platelet-derived growth factors. Stem cell therapy is used for a broader regenerative signaling effect, especially in tougher cases where tissue remodeling is the main goal. |
| Do you use autologous stem cells? | No. Our treatment model uses allogeneic cells only. That means the cells come from carefully sourced donor material and are produced through a controlled laboratory pathway rather than harvested from the patient during the procedure. |
| What types of stem cells do you produce? | Our biotechnology lab produces five types of stem cells: placental, Wharton's jelly, adipose, endometrial, and dental pulp. Selection depends on the clinical program and physician assessment. |
| Will the cells become a new tendon or ligament? | Patients often assume that's the main mechanism, but the more important role is signaling. These cells help shape the healing environment by influencing inflammation, vascular support, and matrix remodeling. |
| Is the procedure surgical? | No. In this setting, treatment is generally performed as an image-guided injection procedure, not an open surgery. Whether that is appropriate depends on the injury pattern. |
| How long does recovery take? | Recovery is usually progressive rather than immediate. The tissue needs time to remodel, and patients typically need an organized rehabilitation plan to support the healing window. |
| Can stem cell therapy replace surgery? | Sometimes, but not always. Some injuries still require surgical repair because the structure itself must be mechanically restored. Regenerative treatment is most useful when the biology of healing is the main limitation. |
| What if I've already tried physical therapy and rest? | That's often the group most interested in regenerative care. If symptoms persist despite appropriate conservative treatment, a more advanced biologic approach may be worth evaluating. |
| Is everyone with tendon pain a candidate? | No. A clear diagnosis comes first. Pain can come from tendon degeneration, tear patterns, referred pain, joint issues, or nerve irritation. The right treatment depends on which of those is actually present. |
| Why does image guidance matter? | Tendons and ligaments are precise structures. Ultrasound guidance helps the physician place treatment at the actual site of pathology instead of relying on surface landmarks alone. |
Article Publication Information
| Field | Content |
|---|---|
| Publisher URL | Longevity Medical Institute Treatments and Resources |
| Author | Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients. |
| Medical Review | Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care. |
| Last Reviewed | May 4, 2026 |
| Disclaimer | This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation. |
If you're considering Longevity Medical Institute for stem cells for ligament and tendon repair, the next step is a formal evaluation focused on diagnosis, tissue quality, and treatment fit. The goal isn't to force every injury into a regenerative plan. It's to determine whether a carefully controlled, allogeneic, image-guided pathway makes clinical sense for your specific case.