Ozone Therapy Benefits: Pain Relief & Advanced Healing
The mention of “ozone therapy” often evokes a simplistic idea: more oxygen must mean better healing. That isn't the most useful way to understand it.
In clinical practice, the more accurate question is whether ozone can act as a controlled biological signal that nudges the body toward better regulation. That's where the conversation becomes more interesting, and more honest. The value of ozone isn't that it functions as a magic fix. It's that, when used correctly, it may help the body mount a more efficient response to inflammation, stress, and recovery demands.
That distinction matters for patients who are trying to separate grounded medicine from exaggerated wellness claims. Some of the most relevant ozone therapy benefits appear in focused areas such as pain support, selected wound-healing settings, and broader bioregulatory care. At the same time, the evidence is still limited in important ways, and route of delivery matters a great deal.
At a premium clinical level, ozone belongs in the category of integrative tools, not stand-alone cures. It's one option within a larger program that may include diagnostics, rehabilitation, metabolic support, and regenerative care. That's also why patients exploring Trifusion ozone therapy should ask not just “Does it work?” but “For which goal, by which method, under whose supervision, and with what trade-offs?”
Rethinking Ozone Therapy for Modern Wellness
What if ozone therapy is less a treatment to "boost oxygen" and more a way to influence how the body regulates stress, inflammation, and recovery?
That is the more useful clinical frame. In modern practice, medical ozone is best understood as a bioregulatory tool. It delivers a controlled physiologic stimulus that may prompt adaptive responses relevant to inflammation, tissue repair, circulation, and resilience. For patients in longevity care, that places ozone in a very specific role. It is an adjunct used to support a broader strategy, not a stand-alone cure.
This distinction helps patients separate plausible medicine from exaggerated wellness claims.
Why the old explanation falls short
The older "oxygenation" narrative is too simple for what clinicians observe. If ozone worked only by delivering more oxygen, outcomes would be easy to predict across patients and indications. They are not. Response depends on the treatment route, dose, timing, and the biology of the patient receiving it.
A better comparison is strength training. The benefit does not come from the stress itself. It comes from how the body responds to a measured challenge. Ozone is studied in a similar way. The therapeutic interest lies in the downstream signaling response, which is why properly administered Trifusion ozone therapy for bioregulatory support is evaluated according to the clinical goal, the delivery method, and the patient's overall plan of care.
That is also where the controversy begins. Mechanistic papers and niche clinical studies suggest possible value in selected settings, while the FDA has warned against unproven medical claims and stresses that ozone is a toxic gas if used improperly. Both points can be true at the same time. There is a biologic rationale worth examining, and there is a clear need for restraint, medical judgment, and professional administration.
Where it fits in a serious program
In a premium longevity setting, ozone usually enters the conversation after the fundamentals are addressed. Sleep, metabolic health, movement, diagnostics, rehabilitation, and inflammatory drivers still come first. Ozone may then be considered when the aim is to support a larger plan for recovery, pain management, vascular support, or delayed healing.
That integrated approach is especially relevant for medical travelers. Patients are often comparing bold marketing claims with mixed regulatory positions and uneven evidence quality. The practical question is not whether ozone is universally "good" or "bad." The practical question is whether a specific modality is appropriate for a specific patient, under trained supervision, with clear goals and realistic trade-offs.
Used that way, ozone therapy belongs in serious medicine as a selective adjunct. Used casually or sold as a cure-all, it does not.
The Science of Cellular Resilience
The best way to understand ozone biologically is to think of it as a cellular workout. Not a destructive one, and not a random one. A brief, controlled challenge.
A good workout doesn't help because the stress itself is pleasant. It helps because the body responds by becoming more capable. Ozone is proposed to work in a similar way. It creates a mild oxidative stimulus that encourages the body to strengthen its own protective systems.
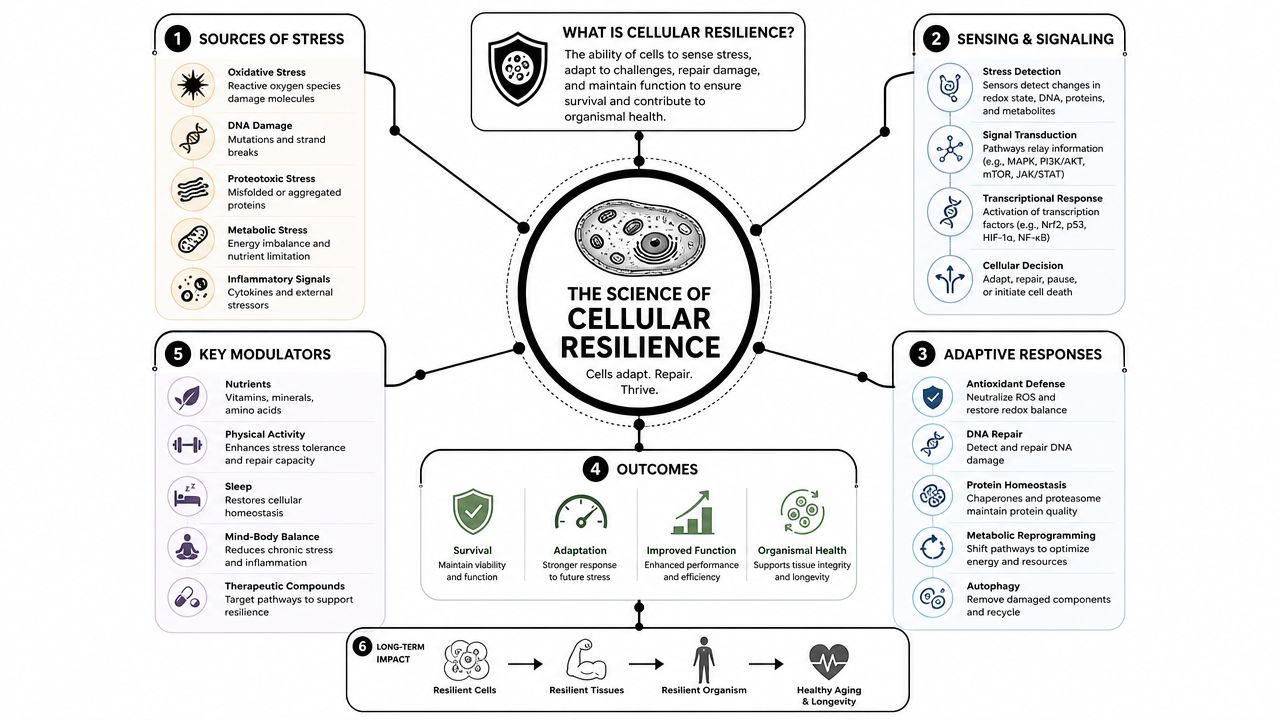
Hormesis in plain language
This principle is called hormesis. A low, controlled dose of stress can trigger adaptation. Too much stress is harmful. Too little challenge produces no useful response. The therapeutic aim is to stay in the adaptive zone.
Mechanistically, reviews describe ozone therapy as a hormetic oxidative stimulus that activates endogenous antioxidant defenses, including the Nrf2 pathway, which then increases antioxidant enzyme production, supports DNA repair, protects mitochondria, and reduces inflammatory signaling, as described in this review of ozone therapy mechanisms and the Nrf2 pathway.
That's why serious clinicians avoid the simplistic phrase “ozone adds oxygen to your body” as the main explanation. The proposed benefit isn't direct oxygen loading alone. It's the downstream response.
Why Nrf2 matters
Nrf2 acts like a cellular control switch for defense and repair. When this pathway is activated appropriately, cells may become better at handling oxidative stress, preserving mitochondrial function, and moderating inflammatory signaling. Those effects are highly relevant in patients dealing with wear-and-tear biology, delayed recovery, or persistent inflammatory burden.
A patient-friendly way to picture this is simple:
The signal: Ozone creates a brief oxidative challenge.
The response: The body upregulates antioxidant and protective pathways.
The payoff: Cells may become more resilient, more efficient, and less reactive.
That's also why ozone is often discussed alongside broader regenerative concepts such as cell regeneration therapy. The therapeutic logic is not about replacing the body's intelligence. It's about provoking a useful adaptive response.
Clinical perspective: The benefit, when it occurs, comes from the body's response to a precise stimulus. That's a very different idea from a cure-all intervention.
What this model does and doesn't support
This mechanism can support careful optimism. It doesn't justify sweeping promises. A plausible biologic rationale is important, but it isn't the same as proof for every condition people mention online.
That's why the strongest conversations around ozone therapy benefits stay focused on areas where the clinical signal is more coherent, rather than trying to force one therapy into every diagnosis.
Evidence-Based Clinical Benefits
The cleanest way to discuss ozone therapy benefits is to separate promising use cases from overreach. The literature doesn't support treating ozone as a universal fix. It does support paying attention to a few niches where the signal is more consistent.
Pain and musculoskeletal support
The strongest evidence appears in pain care. A 2023 systematic review found that ozone therapy's strongest clinical signal is as an adjunct analgesic in pain and musculoskeletal conditions, with a majority of associations supporting reductions in pain (42 associations), low back pain (18), and improved physical function (19) in the mapped evidence, according to the review on ozone therapy for pain and musculoskeletal conditions.
That matters because it narrows expectations. If a patient has chronic low back pain or another musculoskeletal issue, ozone may have a reasonable role as part of a broader plan. If the goal is to replace sound orthopedic evaluation, physical medicine, or conventional treatment, that's where expectations drift away from evidence.
The same review reported no serious adverse effects in the included studies and emphasized that ozone should be considered an integrative option rather than a replacement for standard care. That's exactly how it should be framed in practice.
Vascular and wound-healing settings
A different evidence signal appears in conditions where poor circulation and tissue stress are central problems. Reviews describe potential utility in diabetic foot, ischemic wounds, and peripheral vascular disease, where improved oxygen delivery and antioxidant responses may be clinically relevant, based on this discussion of ozone therapy in inflammatory, vascular, and wound settings.
This is one of the more defensible applications because the biologic logic lines up with the clinical problem. When tissue is struggling under inflammatory load and poor perfusion, therapies that may support local recovery become more interesting. That still doesn't mean ozone works in isolation. Wound care, vascular assessment, infection control, and offloading strategies remain central.
Immune balance, not “immune boosting”
The phrase “immune boosting” is too crude for serious medicine. A better concept is immune modulation. Supporters and some reviews suggest ozone may help with circulation, oxidative stress, and immune-related regulation, while major patient-safety sources also stress that the evidence remains limited.
Here, restraint matters. Some patients do report benefit in chronic inflammatory or recovery settings, but the strongest published support still sits closer to pain and selected vascular or wound contexts than to broad immune claims.
| Condition | Primary Application | Reported Outcomes |
|---|---|---|
| Musculoskeletal pain | Adjunct analgesic support | Reduced pain and improved physical function in evidence mapping |
| Low back pain | Integrative pain management | Favorable signal within musculoskeletal research |
| Diabetic foot and ischemic wounds | Supportive wound and vascular care | Potential relevance where circulation and tissue repair are impaired |
| Peripheral vascular disease | Adjunct bioregulatory support | Mechanistic rationale around oxygen delivery and antioxidant response |
Patients who are evaluating more advanced protocols, including EBOO and ozone-based systemic approaches, should keep one principle in mind: useful evidence exists, but it's strongest in selected lanes, not across every condition that appears in marketing copy.
Modern Ozone Therapy Treatment Modalities
Delivery method changes the entire risk-benefit conversation. That's why one of the most practical questions isn't whether ozone therapy helps, but how it's being administered.
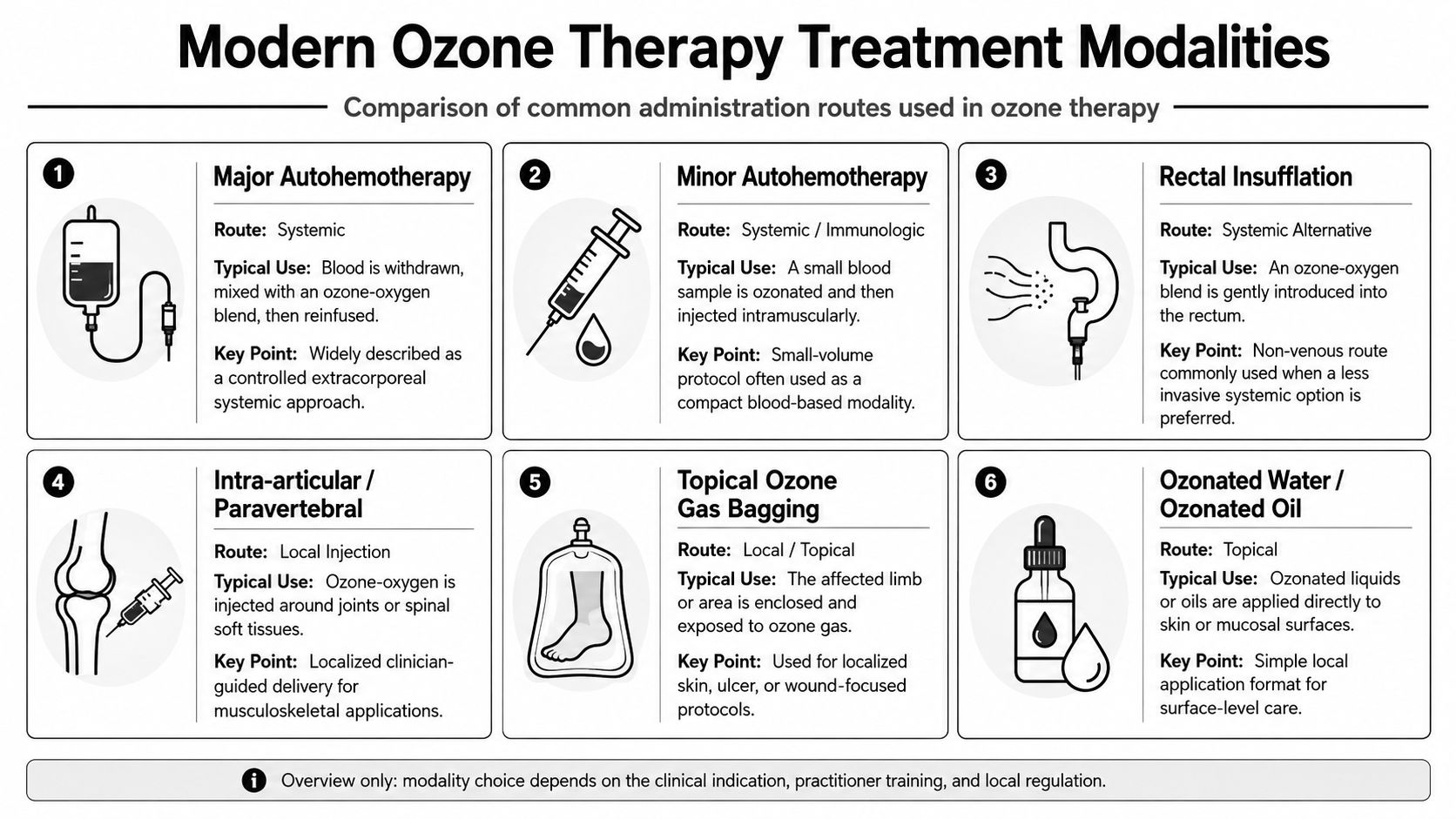
Major autohemotherapy
Major autohemotherapy, often shortened to MAH, is one of the most established systemic methods in integrative ozone practice. Blood is drawn, exposed to a controlled oxygen-ozone mixture in a medical setting, and then reinfused.
Clinicians often favor this method when the goal is a broader systemic effect rather than a purely local one. From a patient perspective, it tends to feel more “medical” and more structured than simpler office-based approaches. It also demands tighter protocol discipline.
Rectal insufflation and topical care
Rectal insufflation is commonly discussed as a less invasive route for systemic intent. It doesn't involve blood handling, which some patients prefer, but it still requires proper dosing and supervision. It should never be treated as a casual or self-directed wellness hack.
Topical applications such as ozonated oils or bagging methods are more localized. These are generally used when the target is skin, soft tissue, or wound support. Their appeal is obvious. They're directed, practical, and often easier for patients to understand. Their limitation is also obvious. They don't substitute for therapies designed for broader systemic action.
Route matters. The expected benefit, the comfort level, and the risk profile all change depending on whether the treatment is systemic, local, or blood-based.
A quick comparison is often more useful than a long technical explanation:
MAH: More procedural, systemic intent, suited to medically supervised programs.
Rectal insufflation: Less invasive, systemic aim, useful when simplicity matters.
Topical ozone applications: Localized support for surface tissues and selected wound scenarios.
For patients who want to see a physician explanation of how advanced ozone-based blood therapies are performed, this overview is useful:
What doesn't work clinically
Unsafe administration undermines the whole conversation. Ozone isn't a therapy to improvise with. Consumer-level devices, vague protocols, and non-medical settings are where confusion and preventable risk creep in.
The method should always match the goal. A patient with localized tissue concerns may not need a systemic route. A patient seeking broad bioregulatory support may not get much from a purely topical one. Good medicine starts by matching indication, route, and protocol.
Integrating Ozone Therapy into Your Longevity Program
Ozone therapy tends to make the most sense when it's used as part of a layered plan. On its own, it may help some patients. Integrated into a broader strategy, it often becomes more clinically coherent.
The reason is simple. Recovery, resilience, and performance don't depend on one pathway. A patient may be dealing with inflammatory burden, poor sleep, deconditioning, mitochondrial strain, unresolved orthopedic mechanics, vascular inefficiency, or all of the above. In that context, ozone is better viewed as one lever among several.
Where synergy matters
In longevity and regenerative medicine, clinicians often use ozone to help create a more receptive physiologic environment. If a patient is inflamed, sluggish in recovery, or stuck in a poor adaptive pattern, a bioregulatory therapy may be useful before or alongside other interventions.
That's where it can pair logically with therapies such as hyperbaric oxygen therapy, which targets oxygen availability from a different angle. These are not interchangeable tools. One is framed as a signaling intervention. The other uses pressure-driven oxygen delivery. In selected patients, those approaches may complement each other.
How clinicians think about combinations
A practical integrated model might look like this:
With rehabilitation: Ozone may support patients whose pain or inflammation limits participation in physical recovery work.
With peptide protocols: Some clinicians pair signaling therapies when the goal is tissue repair support and recovery efficiency.
Before regenerative care: In a physician-led program, ozone may be used to improve the biologic terrain before advanced treatments, including allogeneic cell-based interventions.
At Longevity Medical Institute, ozone therapy is offered within that kind of integrated framework rather than as a stand-alone cure claim. That distinction matters for patients traveling for care because multi-modal medicine usually produces better decision-making than single-therapy marketing.
The right question isn't “Should I do ozone?” It's “Where does ozone fit in my larger plan, and what problem is it meant to solve?”
For some patients, the answer is that it doesn't fit at all. That's an acceptable and sometimes appropriate conclusion. Good care isn't about using every tool. It's about choosing the right ones.
Understanding Safety and Patient Selection
Who should receive ozone therapy, and who should not? That question deserves a clearer answer than wellness marketing usually gives.
In clinical practice, safety depends less on the word "ozone" itself and more on four variables: patient selection, route of administration, dose control, and medical oversight. Ozone can act like a hormetic signal, meaning a carefully controlled exposure may prompt adaptive biologic responses. Poorly selected patients or poorly delivered treatment shift that same intervention from potentially useful to plainly unsafe.
The public debate is confusing because both of these points are true at once. Ozone has been used medically for decades in selected settings, and there is published literature describing low complication rates when trained clinicians use established protocols. At the same time, evidence remains uneven across indications, large high-quality trials are limited, and regulators have warned against unsupported or improper use.
The FDA warning and what it means
Cleveland Clinic notes that the FDA warned against ozone therapy in 2019, that safety and efficacy have not been proven in large human trials, and that inhaling ozone can cause severe and permanent lung damage, according to Cleveland Clinic's patient guide on ozone therapy safety and regulation.
That warning should shape clinical decision-making. It should not be ignored, and it should not be stretched into claims that every medical use is identical. The practical takeaway is straightforward. Inhaled ozone is dangerous, and medical ozone should only be considered through controlled non-inhalation routes, with a defined indication and physician supervision.
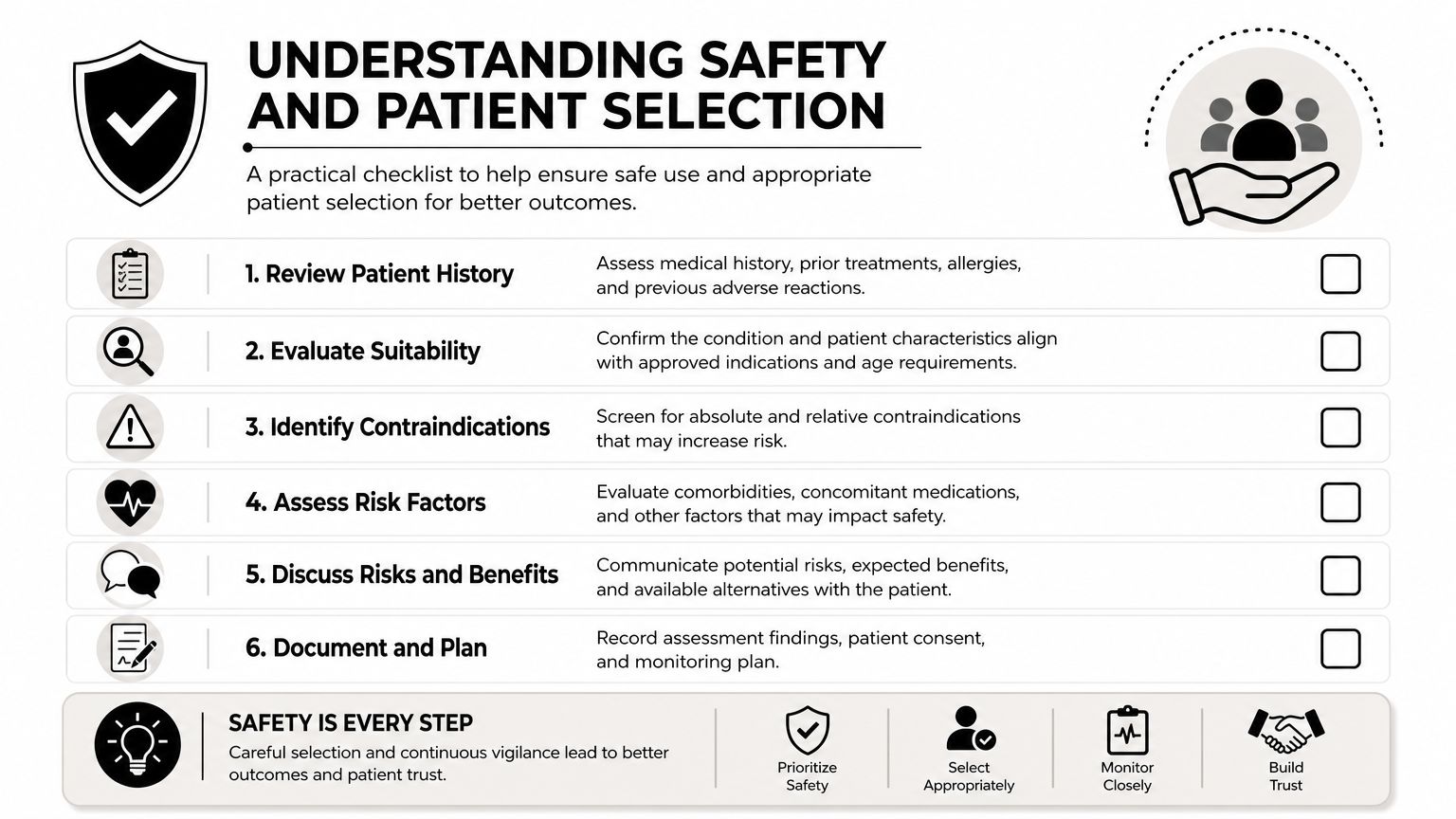
What careful screening looks like
At a premium longevity clinic, screening starts with the clinical objective. Are we trying to support recovery, modulate inflammation, or improve tolerance for another part of the program? If that goal is vague, ozone usually does not belong in the plan.
Patient selection then becomes more specific. Physicians commonly review medical history, current medications, the proposed route, and known contraindications such as G6PD deficiency, pregnancy, and hyperthyroidism. Baseline resilience matters too. A patient with significant oxidative stress burden, unstable medical issues, or unrealistic expectations may be a poor candidate even if no formal contraindication appears on paper.
A useful checklist includes:
A defined indication: The treatment should address a real clinical problem, not a broad promise.
Route matched to purpose: The method used should fit the tissue target and therapeutic goal.
Qualified supervision: Treatment should occur in a physician-led setting with sterile technique and documented protocols.
Clear risk discussion: Patients should understand what is known, what remains uncertain, and why inhalation is not part of proper medical use.
Integration into a larger plan: Ozone should have a role inside a broader strategy, not serve as a stand-alone cure narrative.
This bioregulatory framing matters for medical travelers. A discerning patient should ask not only whether a clinic offers ozone, but how that clinic decides against using it. For that reason, reviewing a clinic's standards for trust, safety, and transparency in patient care is part of due diligence.
Used this way, ozone therapy is neither dismissed reflexively nor oversold. It is treated like any serious medical tool. Useful in selected cases, inappropriate in others, and safest when it sits inside an integrated longevity program with disciplined screening and professional administration.
Frequently Asked Questions About Ozone Therapy
Does ozone therapy replace standard medical treatment
No. The most evidence-based way to use it is as an adjunctive or integrative therapy. It may support a larger plan, but it shouldn't replace appropriate medical evaluation, diagnosis, or conventional treatment when those are needed.
What does a treatment session feel like
That depends on the route. Blood-based and insufflation methods usually feel more procedural than spa-like, while topical applications feel more localized and straightforward. Most patients want to know whether treatment is tolerable, but the more important question is whether the chosen method fits the clinical goal.
Is ozone therapy mainly for pain
Pain is where the clinical signal is strongest in the published evidence discussed above, especially in musculoskeletal care. That doesn't mean pain is the only use. It means it's one of the more grounded places to start the conversation.
Is ozone therapy safe
It can be safe when professionally administered under controlled conditions, but it is not automatically safe in every form. Inhaled ozone is dangerous. Screening, route selection, and physician oversight are central.
How many sessions do patients need
There isn't a one-size-fits-all answer. The appropriate course depends on the indication, the route, the patient's baseline health, and whether ozone is being used alone or inside a larger program. A thoughtful clinic should discuss goals, likely timeline, and stopping points clearly rather than offering a generic package.
Can ozone be combined with regenerative therapies
Often yes, but only when the full treatment plan makes sense medically. Clinicians may combine bioregulatory, oxygen-based, and regenerative therapies when the patient's diagnosis and recovery strategy support that approach.
If you're considering ozone therapy and want a physician-led evaluation of whether it belongs in your care plan, Longevity Medical Institute offers personalized consultations focused on safety, indication, and integrated regenerative strategy.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: June 19, 2026
Short Disclaimer
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.