Stem Cell Therapy for Chronic Fatigue Syndrome: New Hope
Some mornings, people with ME/CFS wake up feeling as if they never slept at all. A shower can feel like a workout. A simple errand can trigger a crash. The hardest part is often that the illness is largely invisible, while its effects shape every hour of the day.
That's why interest in stem cell therapy for chronic fatigue syndrome has grown. Not because it's a magic fix, and not because thoughtful patients are naïve, but because ME/CFS still has no approved curative therapy and many people are left piecing together symptom management, pacing, sleep support, and careful lifestyle adjustments with only partial relief. In that gap, regenerative medicine has become an area of serious attention.
A New Path for Chronic Fatigue Syndrome
ME/CFS changes the scale of ordinary life. Activities that used to feel automatic can become negotiations. You may start planning your week around how much standing, thinking, driving, or social interaction your body can tolerate without tipping into post-exertional malaise.
For many patients, the frustration isn't only physical. It's the sense that the body no longer responds predictably. Rest doesn't reliably restore energy. Effort doesn't produce normal stamina. You can look fine from the outside and still feel as if your internal systems are running on emergency backup.
That's where regenerative medicine enters the conversation. In this setting, stem cell therapy isn't presented as a cure. It's being explored as a supportive, investigational approach for a condition with a major treatment gap. Clinical discussions of mesenchymal stem cells, or MSCs, describe them as tools for immune and inflammatory regulation rather than a replacement for pacing or symptom management.
Why this approach feels different
Traditional ME/CFS care often focuses on managing what the illness does. Regenerative medicine asks a different question. What if part of the problem lies in a disturbed cellular environment, and what if treatment could help calm that environment rather than chase symptoms?
That distinction matters. The target isn't “being tired.” The target is the biology that may be keeping the body stuck in a low-function state.
ME/CFS care works best when hope and realism stay in the same room.
Patients considering treatment abroad often need more than a scientific summary. They need a roadmap. They want to know what stem cells may do, who might be an appropriate candidate, how safety is evaluated, and how to think clearly about travel, clinic standards, and expectations.
Understanding the Biology of Chronic Fatigue
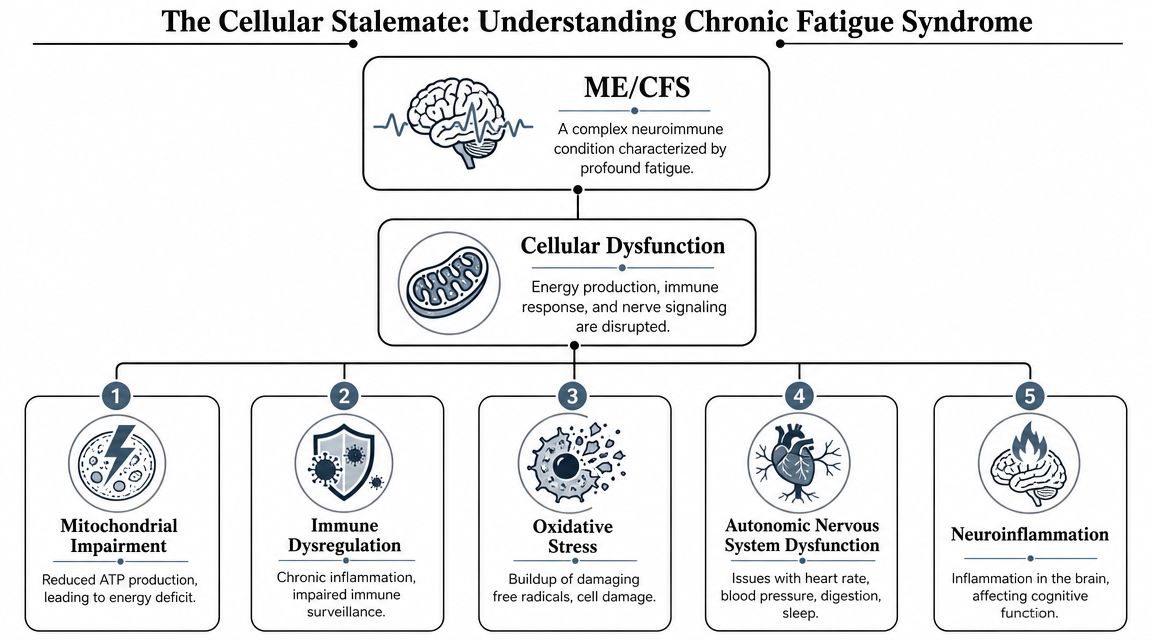
ME/CFS is often described in symptom terms, but symptoms are only the surface. A more useful way to think about the illness is as a cellular stalemate. Multiple body systems appear to be signaling distress at the same time, and none of them fully resets.
The body's energy problem
One way to picture ME/CFS is to imagine a city where the power grid still works, but poorly. Lights flicker. Backup systems keep switching on. Essential services continue, but every demand strains the whole network. That's similar to how many patients describe their energy. They aren't sleepy in the ordinary sense. They feel underpowered.
This is why the biology of fatigue matters. Researchers and clinicians often discuss ME/CFS in terms of impaired energy metabolism, immune dysregulation, inflammation, autonomic imbalance, and neuroinflammation. These don't operate in isolation. They interact.
Three drivers that often confuse patients
Immune dysregulation
The immune system isn't only a defense system. It's also a communication network. When that network stays activated or becomes poorly regulated, the body can remain in a constant low-grade alarm state. Instead of mounting a short, useful response and settling down, it may continue sending “trouble” signals.
That matters because these signals affect far more than infection defense. They can influence sleep quality, pain sensitivity, cognition, and how easily the body tolerates exertion. For a patient-friendly primer on this concept, this overview of immune modulation with stem cells is helpful.
Neuroinflammation and brain fog
Many people with ME/CFS say the cognitive symptoms are as disabling as the fatigue. Word-finding becomes harder. Multitasking feels impossible. Concentration slips. This is one reason clinicians pay attention to the possibility of neuroinflammatory processes. If the nervous system is functioning in an inflamed or overstimulated environment, clarity becomes harder to sustain.
Autonomic and vascular instability
The autonomic nervous system manages background functions such as heart rate, blood pressure, digestion, and basic regulation of stress responses. When this system is unstable, patients may feel dizzy, wired-but-exhausted, unrefreshed after sleep, or unable to recover normally after mild activity.
Practical rule: If a treatment claims to “boost energy” without addressing immune and inflammatory signaling, it probably oversimplifies ME/CFS.
Why biology matters for treatment decisions
A lot of confusion comes from trying to treat ME/CFS as if it were only a problem of low stamina. It isn't. It appears to be a systems-level disorder. That's why regenerative therapies are discussed in terms of signaling, regulation, and recovery support rather than brute-force stimulation.
How Allogeneic Stem Cells Target CFS
When people first hear “stem cells,” they often imagine replacement. They picture new cells moving in like repair bricks and rebuilding what's broken. That image is too simple for ME/CFS.
In this condition, the more plausible role of allogeneic mesenchymal stem cells is not straightforward replacement. It's coordination. A useful analogy is a cellular orchestra conductor. The conductor doesn't play every instrument. The conductor helps the entire system return to rhythm.

What these cells are actually doing
The strongest mechanistic rationale for MSC therapy in ME/CFS is immunomodulation. MSCs can downregulate pro-inflammatory signaling and alter T-cell and innate immune activity, which is biologically plausible in a condition thought to involve immune dysregulation, according to this discussion of MSC immunomodulation in ME/CFS.
That sentence is dense, so let's translate it.
MSCs appear to act more like biological mediators than fuel injectors. They release signaling molecules, often discussed under the umbrella of paracrine signaling, that may help shift the body away from chronic inflammatory overdrive. Think of them as sending calming, organizing messages into a chaotic environment.
Later in the section, this visual helps reinforce the mechanism:
Why allogeneic cells matter
This article focuses on allogeneic cells, meaning donor-derived cells prepared under controlled conditions. In clinical practice, this matters for consistency, quality control, and protocol design. Rather than harvesting from a patient whose own biology may already be under strain, allogeneic therapy aims to use carefully produced cellular products with defined handling standards.
At Longevity Medical Institute's mesenchymal stem cell therapy resource, patients can review how MSC therapy is framed within a broader regenerative strategy. The institute's stated cell platforms include placental, Wharton's jelly, adipose, endometrial, and dental pulp derived cells, produced in its biotechnology lab.
Mechanism in plain language
Here is the simplest way to understand the intended effect.
Immune recalibration helps reduce the background “static” that may be amplifying fatigue, pain, and post-exertional crashes.
Anti-inflammatory signaling may help quiet pathways that keep tissues and the nervous system in a reactive state.
Support for tissue repair may improve the environment around blood vessels, connective tissue, and other stressed systems.
Neurovascular support is relevant because many patients struggle with brain fog, dizziness, and effort intolerance.
These effects are expected to unfold over time, not instantly.
A short comparison
| Common assumption | More accurate explanation |
|---|---|
| Stem cells replace damaged tissue directly | In ME/CFS, the likely benefit is signaling and regulation |
| Treatment should work right away | Biological response may take weeks to months |
| More cells always means better results | Standardization, patient selection, and protocol design matter more |
The goal isn't to force energy into the body. It's to improve the cellular environment so the body can regulate itself more effectively.
Why this still remains investigational
Even with a sound mechanistic rationale, stem cell therapy for chronic fatigue syndrome is still experimental. Studies remain limited, and the field still needs better standardization around cell source, dose, route, and endpoints. That's why thoughtful clinics speak in terms of possibility and monitoring, not certainty.
Evaluating Clinical Evidence and Safety
A patient considering treatment abroad has to weigh two questions at the same time. Could this therapy help, and how do I judge whether a clinic is handling it responsibly?
For ME/CFS, the evidence for mesenchymal stem cell therapy supports careful interest, not cure claims. That may sound cautious, but it is protective. Chronic fatigue syndromes are complex, the research base is still developing, and patients who travel for care need clear expectations before they book a flight, transfer records, or commit to a protocol.
What the clinical evidence actually shows
The published literature is still early. Most reports suggest a pattern rather than a final answer. Some patients describe improvement in fatigue, mental clarity, sleep, pain, and daily function after MSC treatment, which fits the symptom burden clinicians are trying to address. A review in Stem Cells International also describes MSCs as a therapy being studied for their immunomodulatory and anti-inflammatory effects across chronic inflammatory conditions, which helps explain why they remain of interest in illnesses such as ME/CFS (review of mesenchymal stem cell mechanisms and clinical safety).
That said, early signals are not the same as proof.
Why interpretation is difficult
ME/CFS research often runs into the same problem as trying to compare several maps drawn at different scales. Each one may contain something useful, but they do not line up perfectly.
Small patient groups: Many reports are based on limited numbers, which makes it hard to know how broadly the results apply.
Different treatment methods: Cell source, dose, timing, and infusion approach vary from one program to another.
Symptoms that are hard to measure: Fatigue, post-exertional worsening, and brain fog are real clinical problems, but they are harder to quantify than a lab value.
Mixed patient populations: Post-viral illness, longstanding ME/CFS, dysautonomia, and Long COVID overlap, yet they may not respond in the same way.
This is why a serious clinic should speak in terms of probability, monitoring, and patient selection. A trustworthy conversation sounds measured, especially in medical tourism, where distance can make glossy promises harder to verify.
Safety is a system, not a single claim
Patients often hear that stem cell therapy is "safe," but safety in regenerative medicine works more like an airport security chain than a single checkpoint. The final infusion matters, yet the steps before it matter just as much. Donor eligibility, infectious disease screening, cell handling, storage, transport, physician oversight, and post-treatment follow-up all shape real-world risk.
| Safety layer | Why it matters |
|---|---|
| Cell sourcing | Affects consistency, donor screening, and contamination risk |
| Processing controls | Helps preserve product integrity and sterility |
| Medical screening | Identifies patients who may need other evaluation before treatment |
| Follow-up | Tracks delayed reactions and meaningful functional change over time |
For readers comparing clinics, this explanation of questions to ask about stem cell therapy safety is a useful starting point.
A regulated medical setting cannot promise a specific outcome. It can improve screening, documentation, product controls, and adverse-event oversight, which lowers preventable risk.
What safety means for medical tourists
This matters even more when treatment involves travel to Mexico or another international destination. A clinic may advertise the same cell type as another center, yet the patient experience can be very different depending on how records are reviewed, how candidacy is determined, whether the physician explains contraindications clearly, and what happens if symptoms flare after you return home.
For US and Canadian patients, good safety planning includes practical details. You should know who is responsible for pre-travel review, what testing is required before arrival, how infusion day is supervised, what short-term side effects are expected, and how follow-up is handled once you are back home. In other words, the safety question is never just "What is in the syringe?" It is also "What system surrounds the treatment?"
What honest communication sounds like
If a clinic describes stem cell therapy for chronic fatigue syndrome as a guaranteed reset, that is a warning sign. If the clinic explains that the therapy is investigational, that response patterns vary, and that the goal is support rather than a definitive cure, the message is much closer to current evidence.
That kind of honesty helps patients make better decisions. It also helps them travel with realistic expectations, which is one of the most important protections in cross-border care.
Your Treatment Journey at Longevity Medical Institute
For medical tourists, the treatment journey matters almost as much as the treatment itself. The quality of evaluation, preparation, monitoring, and follow-up often determines whether the experience feels coherent or confusing.
A serious protocol for chronic fatigue doesn't begin with a bag of cells. It begins with selection. Intravenous infusion is a common route, but outcomes depend on careful patient selection and an understanding that the intended effect is transient signaling over weeks to months.

Step one is ruling things in and out
A premium regenerative program should not assume every exhausted patient has ME/CFS, and it shouldn't assume every ME/CFS patient is a candidate for stem cells.
That first stage usually includes a detailed review of medical history, current symptoms, prior diagnoses, medications, infection history, autonomic symptoms, sleep quality, and functional limitations. In more developed programs, clinicians also use broader diagnostics to identify competing or contributing issues such as endocrine dysfunction, nutritional problems, inflammatory patterns, or cardiometabolic concerns.
What a thorough workup often includes
Clinical review: Symptom pattern, onset history, and major triggers.
Laboratory assessment: A broad biomarker panel to identify inflammation, immune irregularities, and other fatigue drivers.
Imaging when indicated: Advanced imaging can help rule out unrelated pathology and give a more complete health picture.
Risk screening: The team looks for reasons to delay treatment, modify the protocol, or recommend another path.
What treatment day usually looks like
Once a patient is cleared, the core procedure commonly involves intravenous administration of allogeneic MSCs. The logic is not that these cells permanently engraft everywhere they go. The expected role is signaling. They travel through the circulation, respond to inflammatory cues, and release molecules that may help organize a calmer repair response.
For some patients, physicians may integrate supportive therapies that complement a regenerative plan. Depending on the clinic, that can include targeted oxygen-based recovery strategies, restorative medical oversight, and structured post-treatment observation.
Recovery support matters
The post-infusion period is where many patients get confused. Some expect immediate clarity. Others worry if they don't feel different right away. Both reactions are common.
A thoughtful care pathway usually includes:
Observation after treatment so the medical team can monitor tolerability.
Guidance for the following days around activity, hydration, rest, and symptom tracking.
Planned follow-up focused on function, not just impressions.
The most useful question after treatment isn't “Do I feel dramatically different today?” It's “Is my capacity changing over time?”
Why this process needs coordination
ME/CFS is a systems-level illness, so treatment should be organized the same way. A fragmented experience, where one clinic infuses cells and leaves the patient to interpret everything else alone, usually creates anxiety and poor expectation management. Patients tend to do better when the process is structured, conservative, and medically supervised from evaluation through follow-up.
Navigating Treatment in Mexico Safely
Traveling for care can be practical and appropriate. It can also expose patients to uneven standards if they don't know what to look for. That's especially important with stem cell therapy, where marketing language often sounds similar from one clinic to another while the underlying quality can differ dramatically.
A recent review of regenerative approaches for post-viral fatigue noted a major real-world problem. Safety and regulatory variability across countries are often under-discussed, even though that issue is central for patients considering cross-border care.
What regulation means in practice
Patients often hear terms like COFEPRIS, ISO certification, in-house lab, and quality control without being told why they matter. In plain language, these markers are meaningful because they speak to accountability.
A practical checklist
Clinic licensing: You want evidence that the medical facility operates under recognized regulatory oversight.
Laboratory standards: If a clinic uses an in-house biotech lab, ask how cell processing and quality control are managed.
Traceability: The clinic should be able to explain sourcing, handling, and release criteria clearly.
Medical supervision: There should be an identifiable physician-led process, not just a sales pipeline.
For patients weighing this decision, this guide to whether stem cell therapy in Mexico is safe offers a useful framework for vetting clinics.
Questions worth asking before you book travel
Not every important question is glamorous, but each one protects you.
| Ask this | Why it matters |
|---|---|
| Who evaluates candidacy medically? | Screens out poor-fit cases |
| Where are the cells produced and how are they handled? | Helps assess product quality |
| What monitoring happens after infusion? | Shows whether the clinic takes follow-up seriously |
| How do they talk about outcomes? | Honest clinics avoid miracle language |
If a clinic makes treatment sound easy but makes safety hard to verify, pause there.
Medical tourism works best when the logistics are simple and the standards are not.
Realistic Outcomes and Recovery Timeline
You return home after treatment hoping for a clear signal that something has changed. What often happens instead is quieter. A shower leaves you less drained. Reading feels possible for 20 minutes instead of 10. The next morning, the crash you expected does not hit as hard.
That pattern matters. In ME/CFS, improvement often shows up as better stability before it shows up as more energy. Stem cell therapy, when it helps, usually works more like resetting a misfiring control system than flipping on a dead battery. Immune signaling, inflammation, sleep quality, and post-exertional recovery can shift at different speeds, so progress rarely arrives in a straight line.
According to a published summary from the Stem Cell Medical Center, clinic-reported experience in patients with chronic fatigue and Long COVID included improvement in up to 80% of treated patients, with changes sometimes reported within 3 to 4 weeks and treatment stays commonly lasting 10 to 14 days in more intensive international protocols. These are clinic-reported figures, not results from large randomized trials, so they are better used as orientation than prediction.
For medical travelers, that distinction is more than academic. It helps you plan realistically. You may need extra rest days after flying, help with airport transfers, and a realistic work re-entry plan once you are back in the US or Canada. The treatment window is only one part of the timeline. Recovery also includes what happens after you leave the clinic.
What patients may notice first
Early changes are often small but meaningful:
Less severe post-exertional crashes: The same activity may still cost energy, but the fallout may be shorter or less intense.
Better cognitive endurance: Concentration, word-finding, or screen tolerance may improve before physical stamina does.
More stable sleep: Sleep may feel deeper or slightly more restorative, even if total energy is still limited.
Fewer pain or flu-like flares: Some patients notice a reduction in the “sick” feeling that often accompanies overexertion.
More reliable baseline function: Ordinary tasks may require less recovery time.
These changes can be easy to miss if you are waiting for a dramatic turning point.
Why pacing still matters after treatment
A calmer immune environment does not instantly erase the body's habit of overreacting to exertion. The safer mindset is to treat early improvement like a green shoot in dry soil. It is encouraging, but it still needs protection. Patients often do better when they keep pacing, guard sleep, hydrate well during travel, and avoid testing their limits too quickly because one good day can be misleading.
At Longevity Medical Institute, this is one reason aftercare planning matters for out-of-town patients. The practical question is not only, “Did I get treatment?” It is also, “How will I protect any early gains once I am back in my normal routine?”
A grounded way to measure progress
Track what changes in daily life, not just how you feel in one moment:
Function: Are basic activities more manageable?
Mental stamina: Can you read, work, or hold conversation longer without payback?
Recovery: Are crashes less frequent, shorter, or less severe?
Consistency: Are improvements repeating often enough to trust them?
For a broader view of what the healing period can look like after treatment, this guide to recovery time after stem cell injection offers helpful context.
Improvement in ME/CFS often looks like the return of predictability. That can be emotionally significant. A body that feels less chaotic is often the first real sign that healing may be underway.
FAQs for US and Canadian Patients
Why do patients travel internationally for this therapy
Many patients travel because access, protocol design, and regulatory pathways differ across countries. That doesn't automatically make international care better or worse. It means the burden is on the patient to verify standards carefully.
Is stem cell therapy for chronic fatigue syndrome approved as a cure
No. It remains investigational for ME/CFS. The most responsible way to view it is as a supportive regenerative option being explored for immune and inflammatory regulation in a condition with limited conventional treatment options.
Are allogeneic cells generally well tolerated
In regulated medical settings, MSC therapy is generally described as well tolerated with low immune reactivity. That said, “well tolerated” doesn't mean “appropriate for everyone.” Candidacy still matters.
How should I evaluate a clinic from abroad
Start with the basics. Ask who performs the medical evaluation, how candidacy is decided, what laboratory controls are in place, how follow-up works, and whether the clinic explains limitations as clearly as benefits.
A strong clinic should answer practical questions directly, including:
What cells are being used: The source and type should be clearly identified.
How safety is monitored: There should be a defined observation and follow-up process.
What outcomes are realistic: Trustworthy teams avoid guarantees.
How travel is handled: International patients need a coordinated plan, not just a procedure date.
What about cost
Costs vary by clinic, protocol complexity, supportive therapies, travel needs, and duration of stay. Because pricing structures differ, the most useful question isn't “What's the cheapest option?” It's “What medical and laboratory standards am I paying for?”
Will I need ongoing care after treatment
Usually, yes. Even when regenerative therapy is part of the plan, patients often still need pacing, symptom management, medical follow-up, and a strategy for measuring function over time.
If you're exploring treatment options and want a medically guided next step, Longevity Medical Institute publishes educational resources for patients considering regenerative and longevity care through its treatment library at Treatments & Resources. A consultation can help determine whether stem cell therapy for chronic fatigue syndrome fits your clinical picture, travel needs, and safety priorities.
Author
Dr. Kirk Sanford, DC, Founder & CEO, Longevity Medical Institute. Dr. Sanford focuses on patient education in regenerative and longevity medicine, translating complex therapies into clear, practical guidance for patients.
Medical Review
Dr. Félix Porras, MD, Medical Director, Longevity Medical Institute. Dr. Porras provides clinical oversight and medical review to help ensure accuracy, safety context, and alignment with current standards of care.
Last Reviewed: May 25, 2026
This information is for educational purposes only and is not medical advice. It does not replace an evaluation by a qualified healthcare professional. For personalized guidance, please schedule a consultation.